
When a patient is discharged from the hospital, it signifies that there is improvement in his/her health and is fully or almost back to normal. But have you ever wondered how doctors and other members of the medical care team make sure that the medical care given to patients is properly recorded? They do this by using a discharge summary template. Here’s how you can create it.
Contents
Discharge Summary Templates
What is a discharge summary from a hospital?
A discharge summary template plays an important role in maintaining the safety of patients after getting discharged from the hospital. The summary serves as the main document that communicates the care plan of a patient to the post-hospital healthcare team.
In most cases, a hospital discharge form is the only document that accompanies a patient to the next stage of medical care. Well-written discharge summaries are typically considered important when promoting safety when a patient transitions between care settings, especially during the initial post-hospital period.
The doctor can test a patient’s understanding through the use of “teach-back.” This is a simple yet essential technique that involves asking patients to explain the instructions to the doctor that he/she just told a patient. Through this technique, a patient comes to know the names of the people responsible for his care upon discharge.
Discharge Summary Samples
What should be included in discharge instructions?
It is true that the development of e-solutions has vastly helped improve communications regarding patient information as they move from one health setting to another. But the use of these new resources cannot ignore the significance of a discharge summary template.
It is still critically important to have it successfully planned and executed by the hospital to help the recovery and the fulfillment of post-discharge healthcare. Before a patient leaves the hospital, he will have a discharge conversation with the discharging nurse and attending clinician.
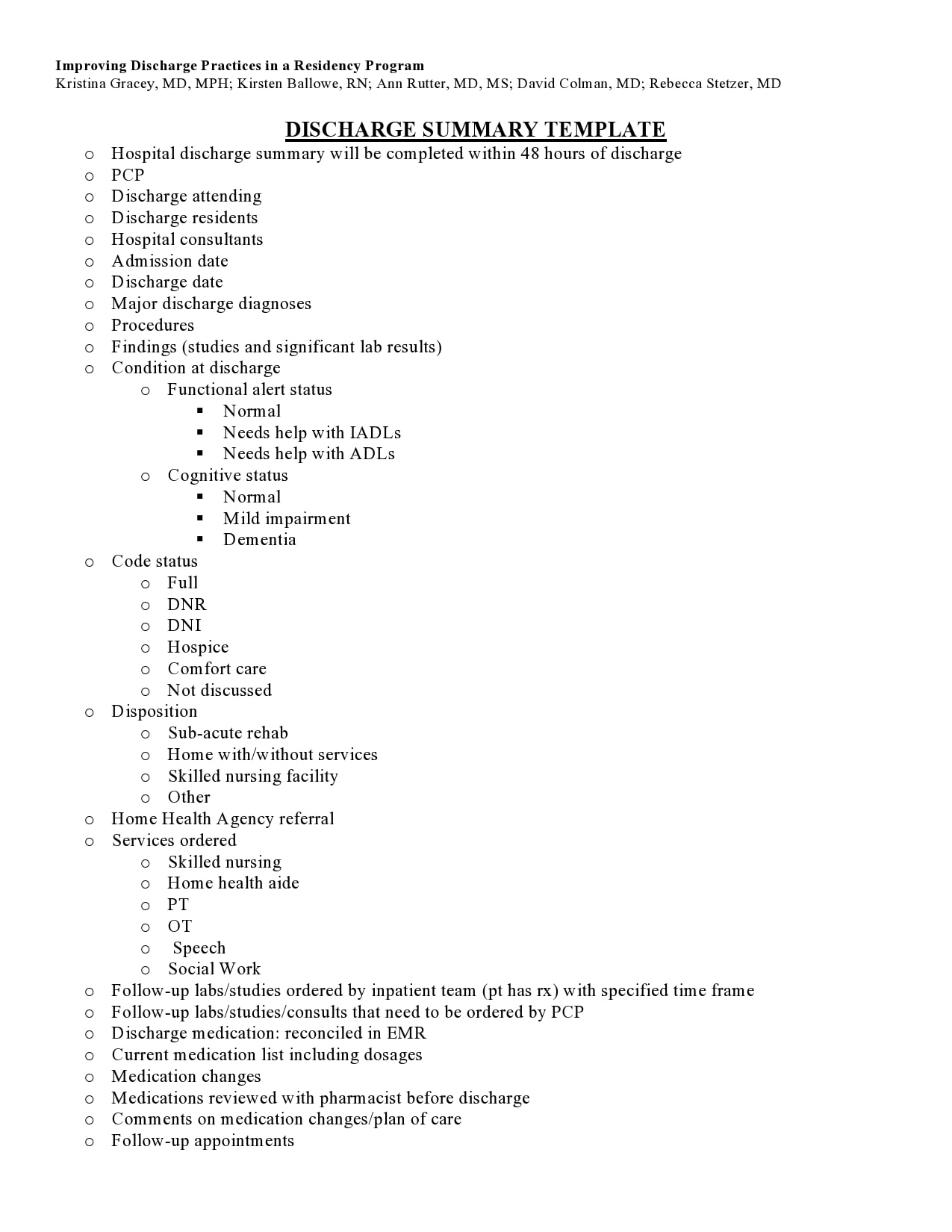
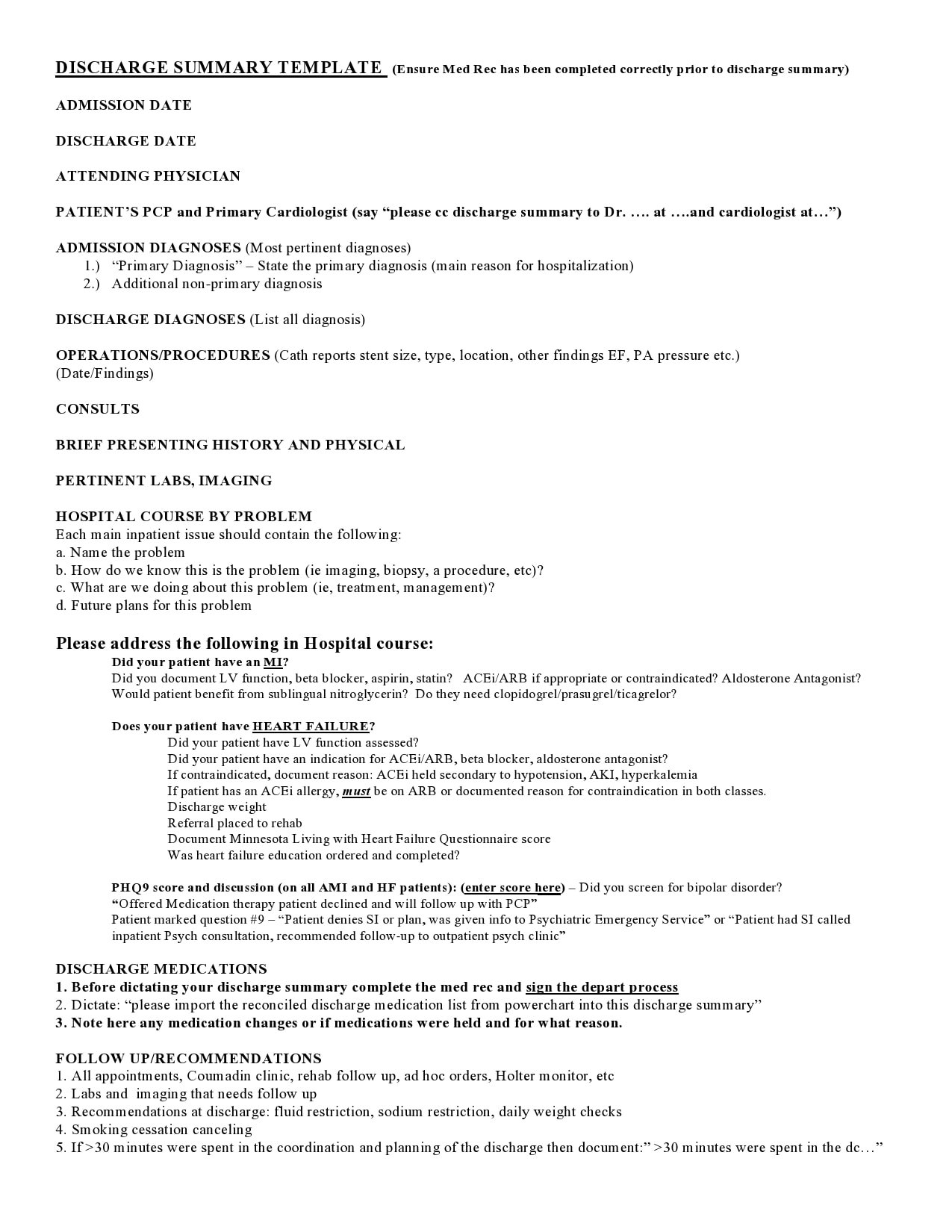
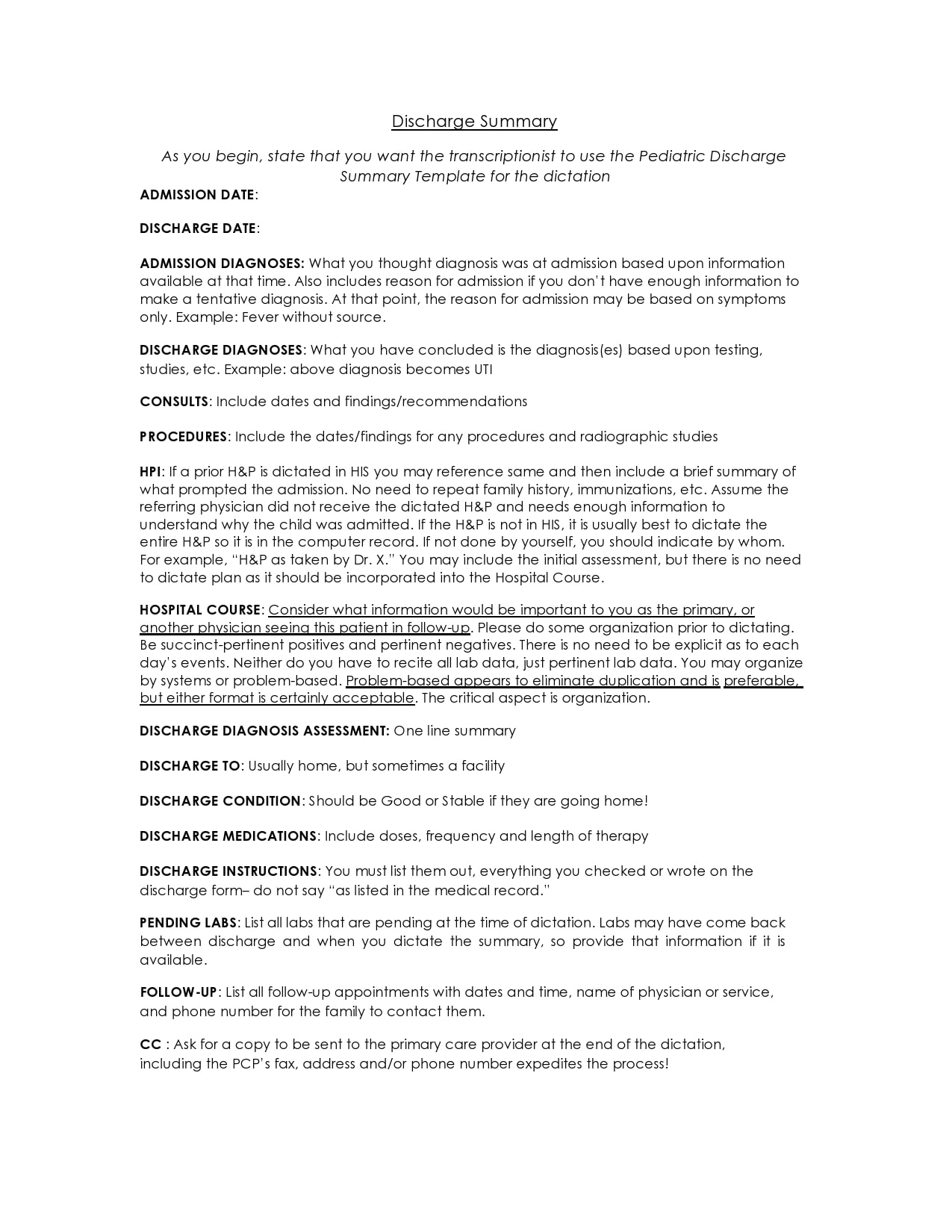
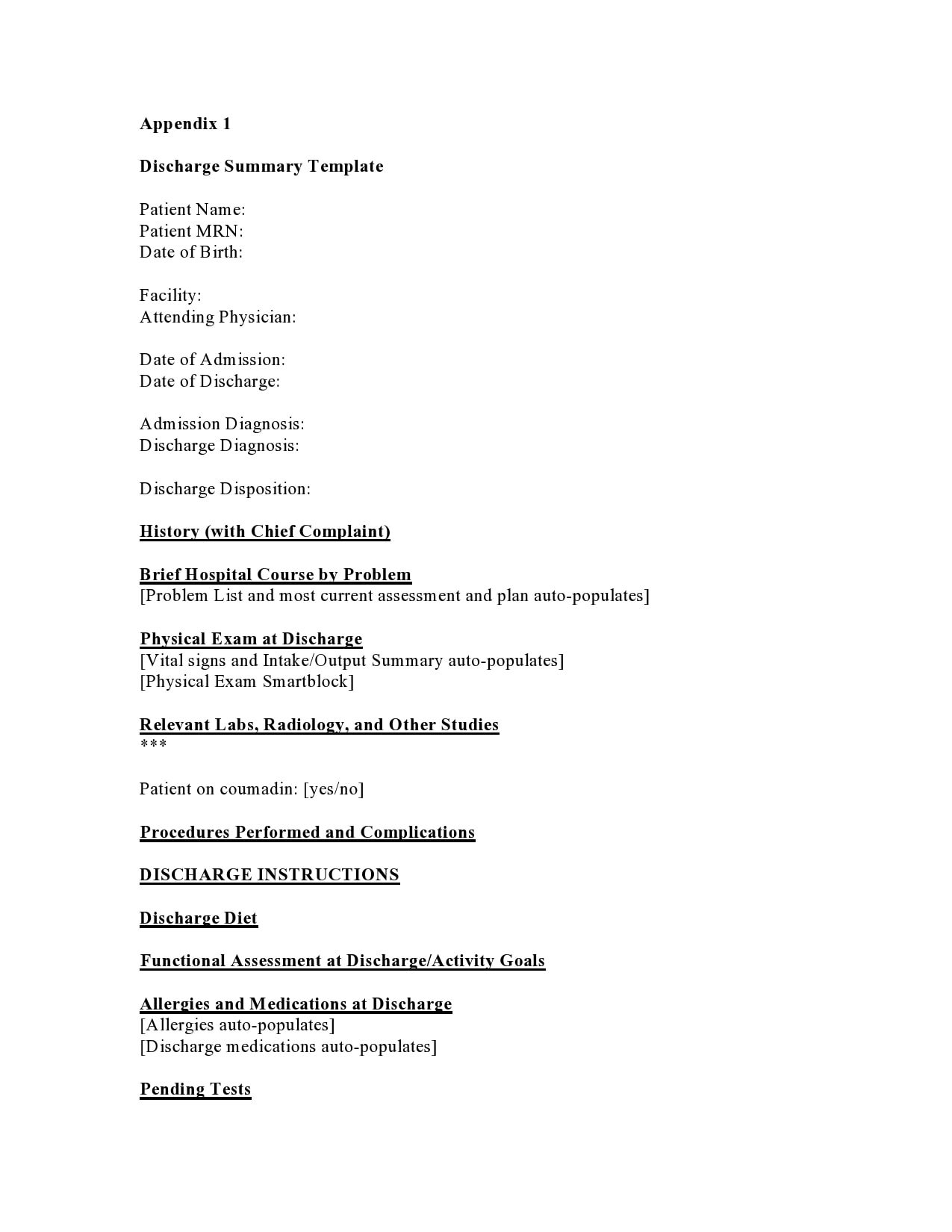
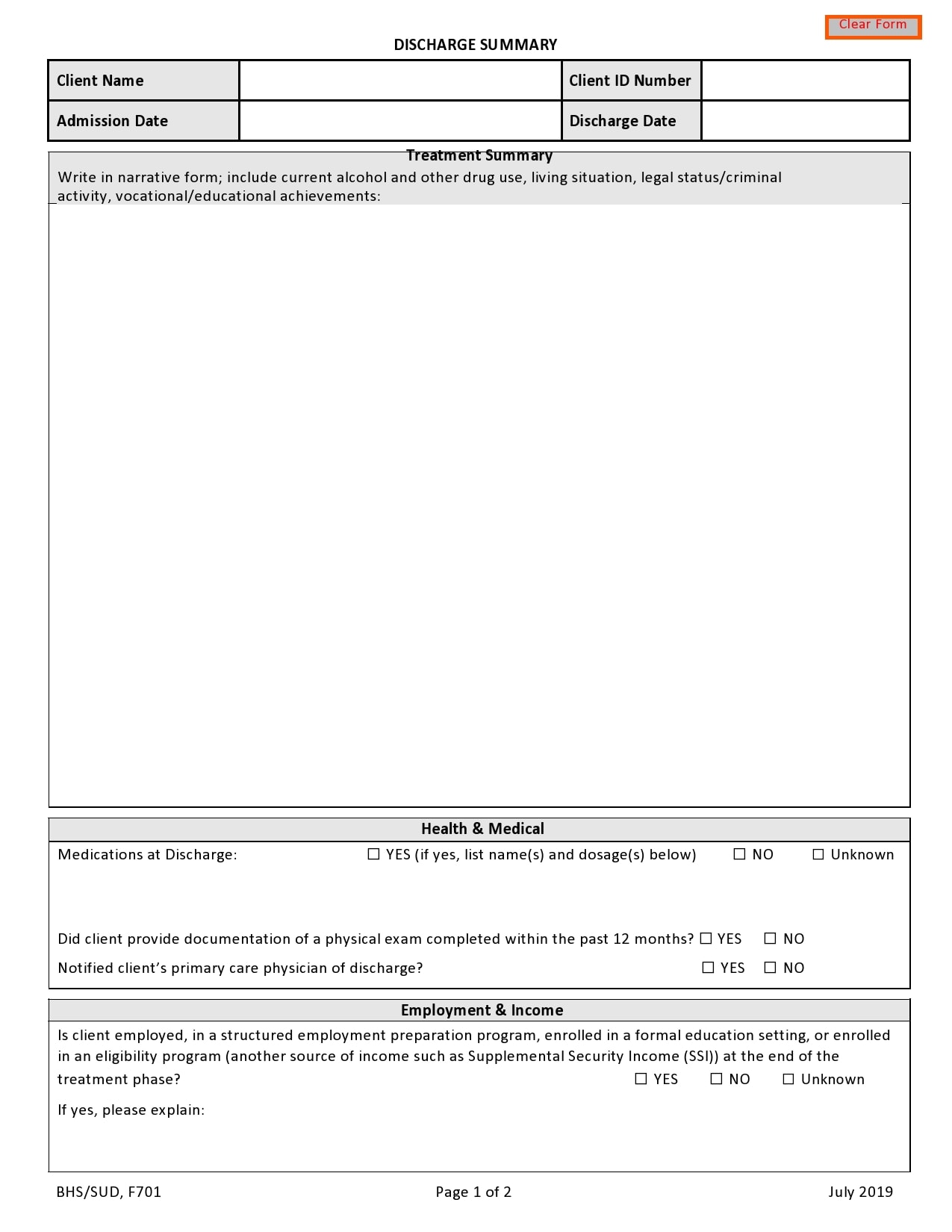
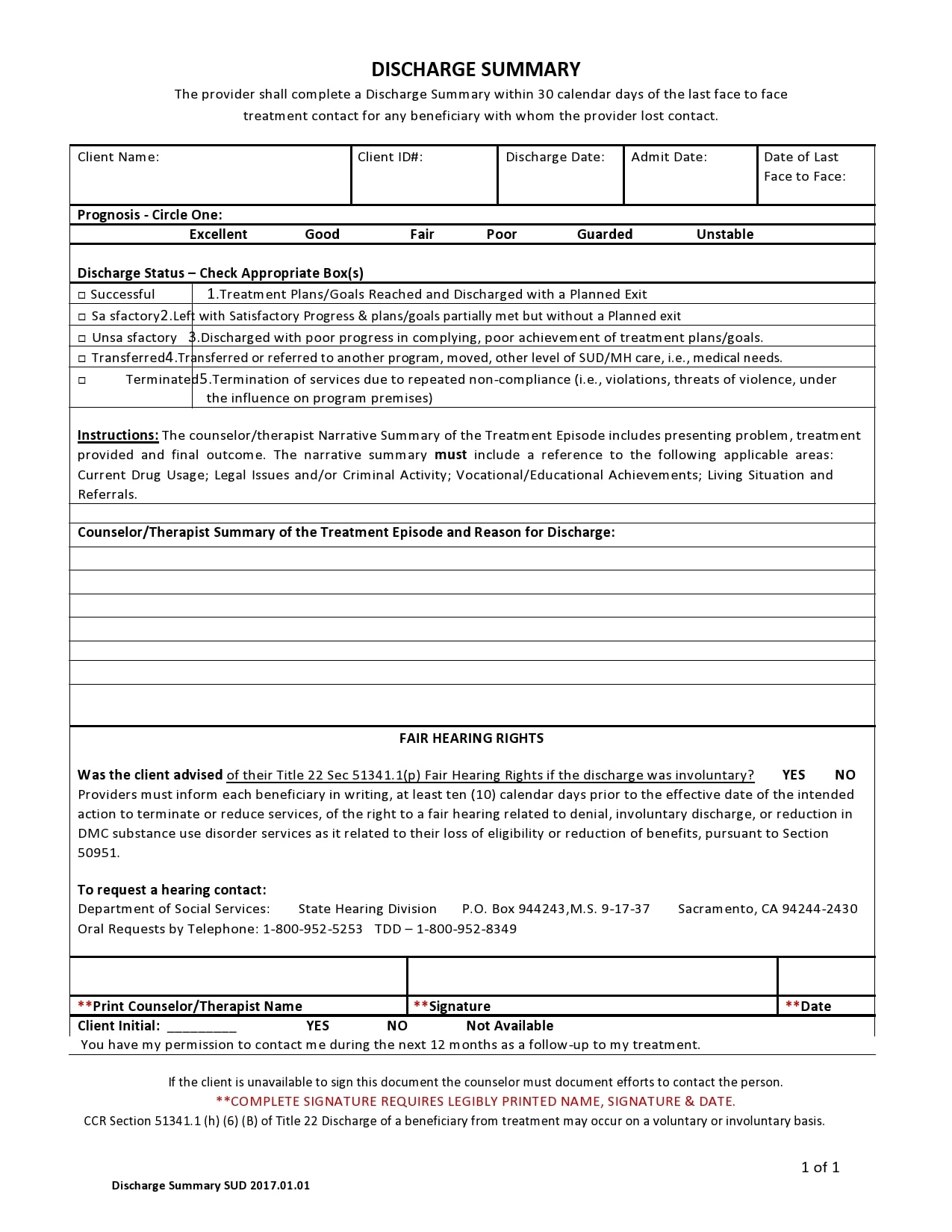
This conversation includes all pertinent information necessary to ensure a patient’s safe departure from the hospital along with proper follow-up. The patient should also have a caretaker, family member, home healthcare provider or a close friend engaged in this conversation. Then the discharge summary sample a patient receives must contain the following:
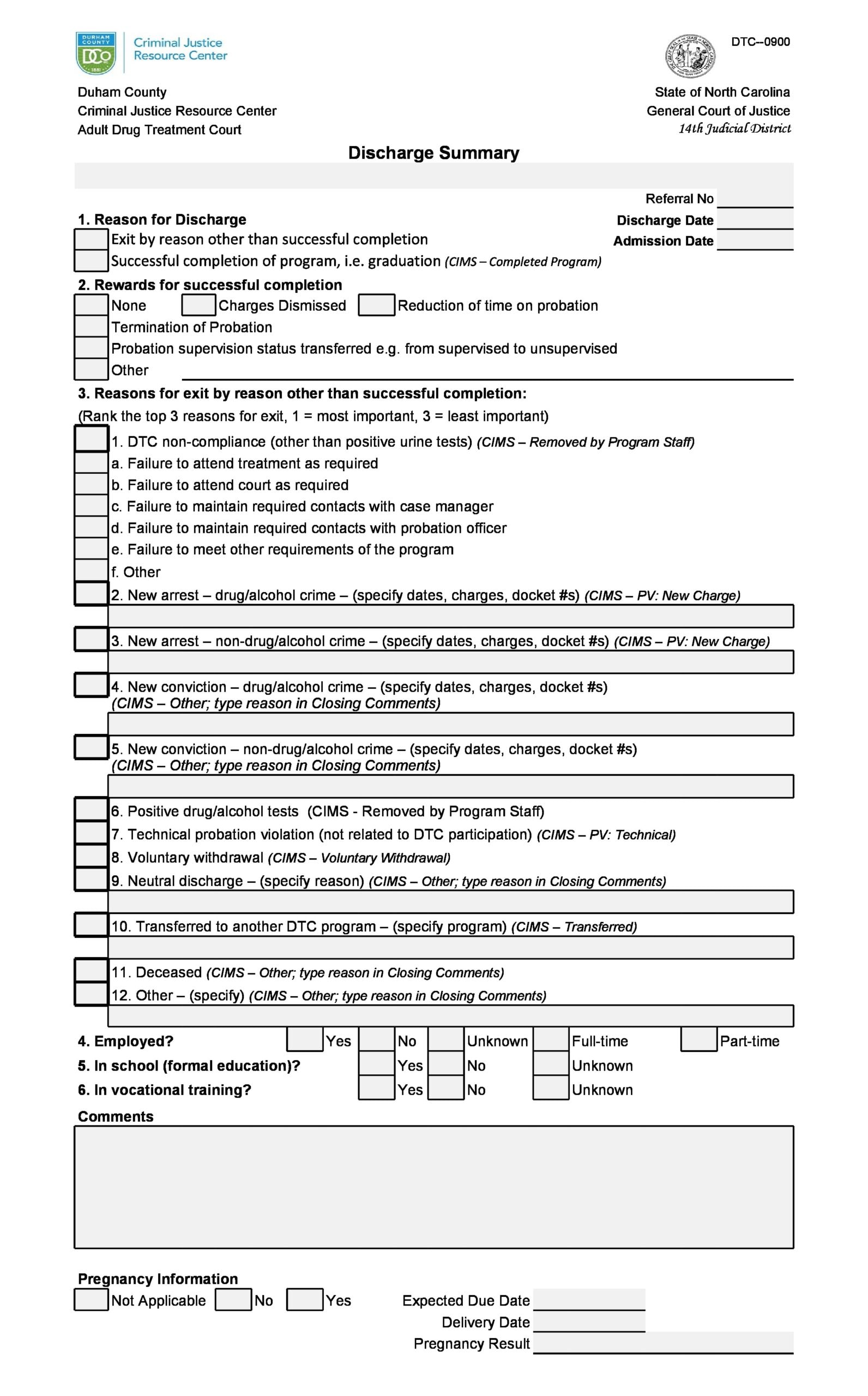
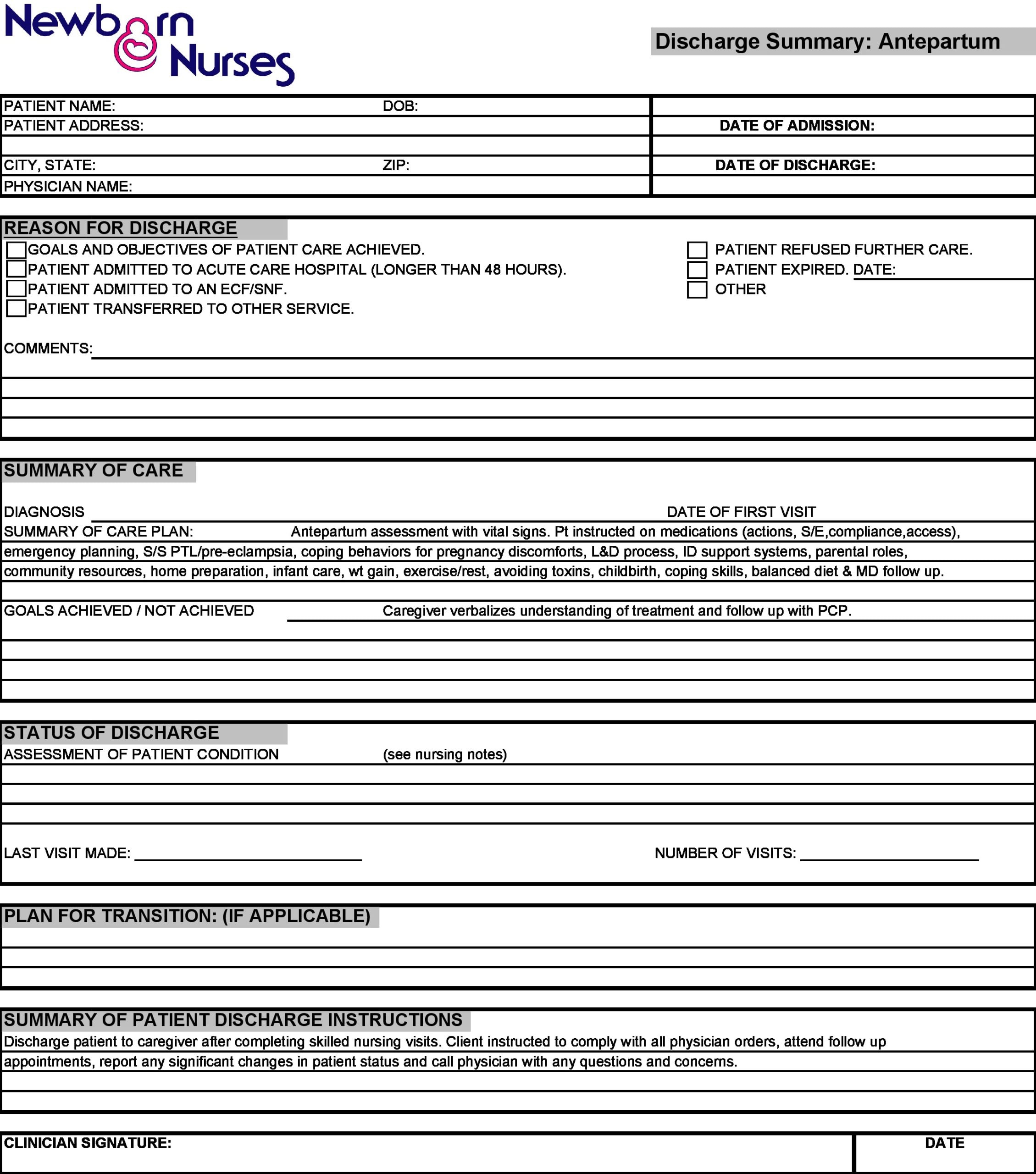
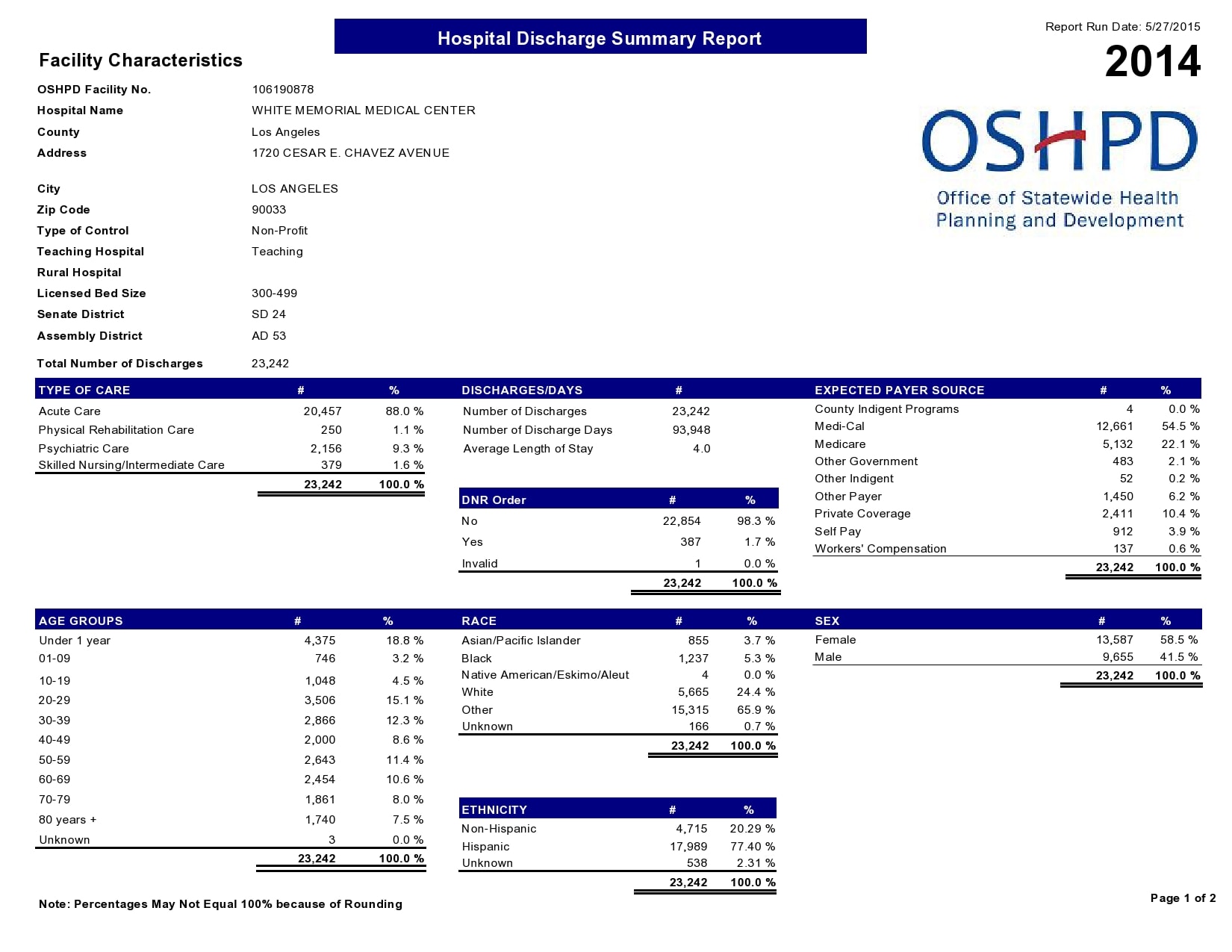
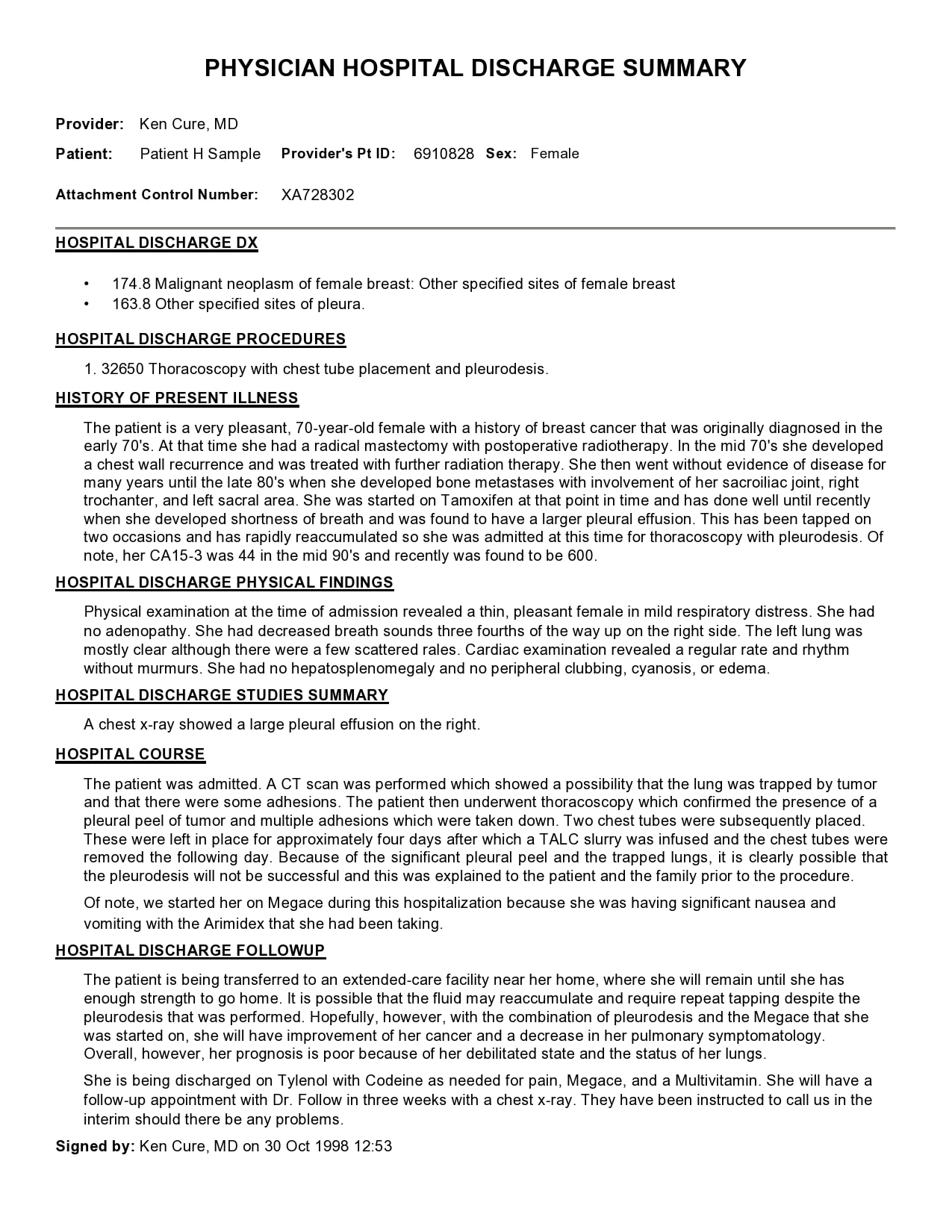
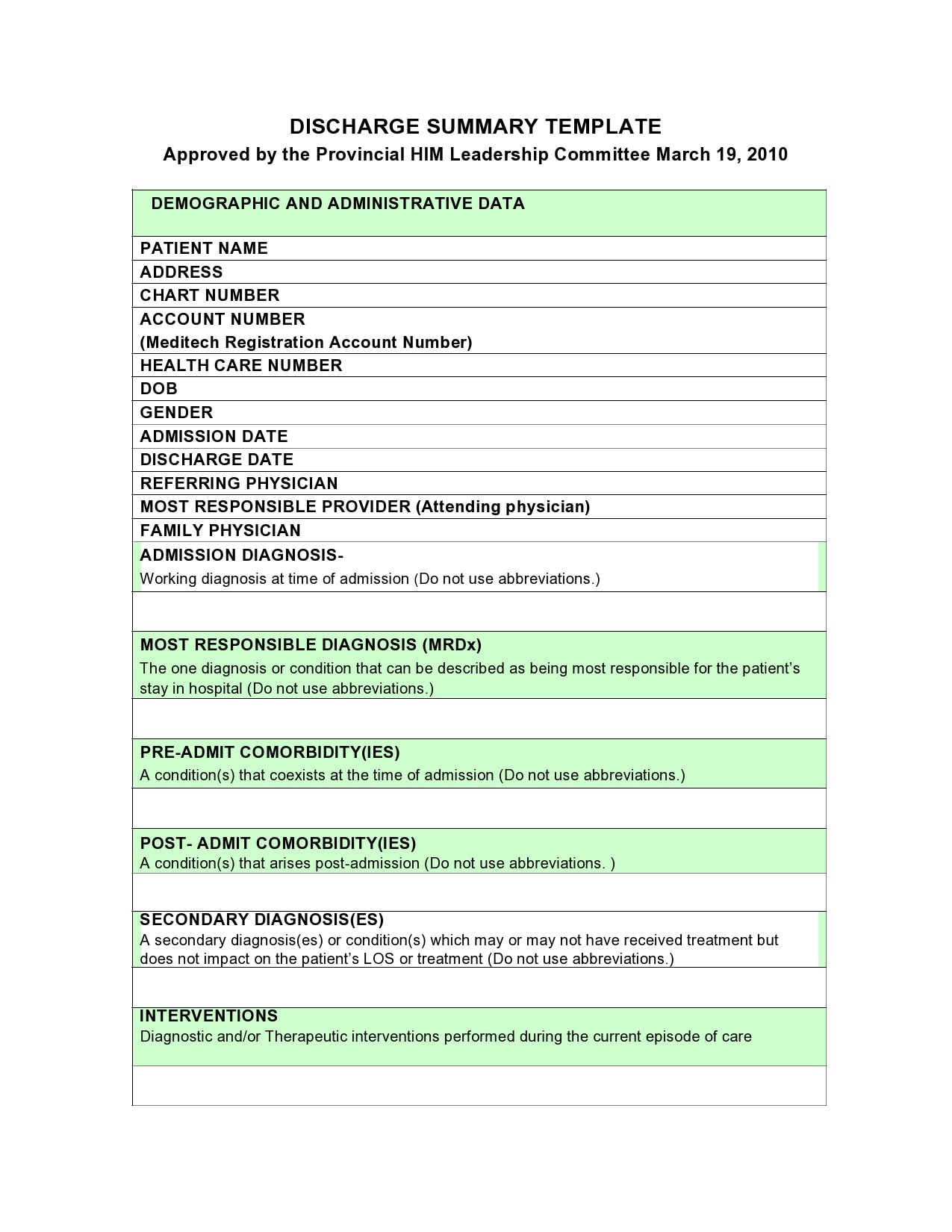
- The reason why a patient got hospitalized
This refers to a description of primary presenting condition or a description of initial presentation to the hospital admission along with a description of initial diagnostic evaluation. - Significant findings
These refer to the doctor’s primary diagnoses. - The procedures done and the treatment provided
This refers to a description of the events that occurred during hospital stay or a description of medical, surgical, allied health consults or other specialties that patient has experienced. It may also refer to a description of invasive, surgical, noninvasive, technical or diagnostic procedures the patient experienced. - Patient’s condition upon discharge
Apart from the patient discharge form template, this refers to any documentation that gives a description of how the patient doing at discharge or the overall health status upon discharge. - Instructions the patient must follow
These refer to any discharge medications, activity orders, dietary instructions, therapy orders or medical follow-up instructions. - Signature of the attending physician
The attending physician must affix their signature on the document to make it official.
Patient Discharge Form Templates

How do you write a discharge summary?
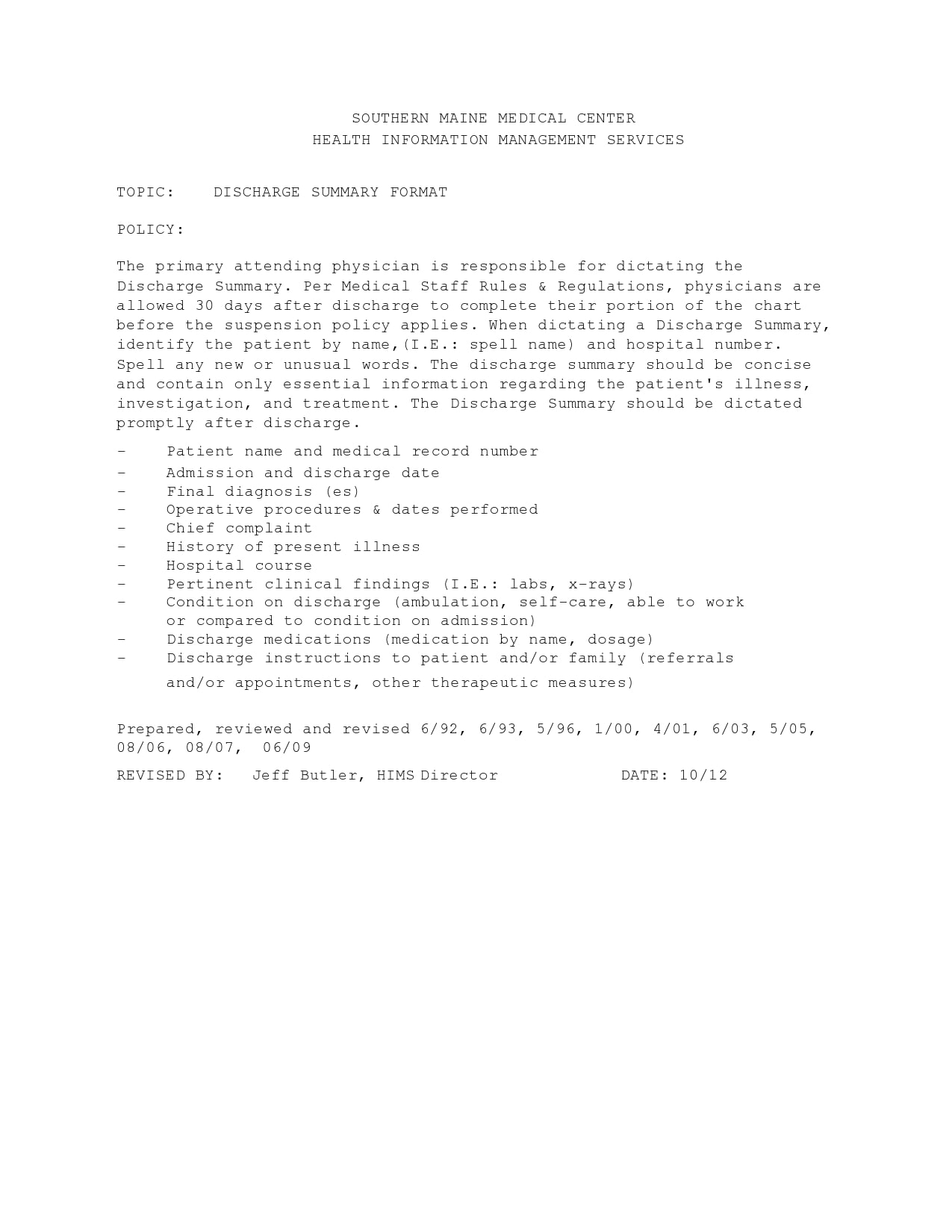
Discharging a patient from the hospital involves a lot of complex work and one of the essential parts of the process is the creation of the discharge plan example. A discharge summary template is a medical report written by a health professional after treatment or at the end of the patient’s stay in the hospital.
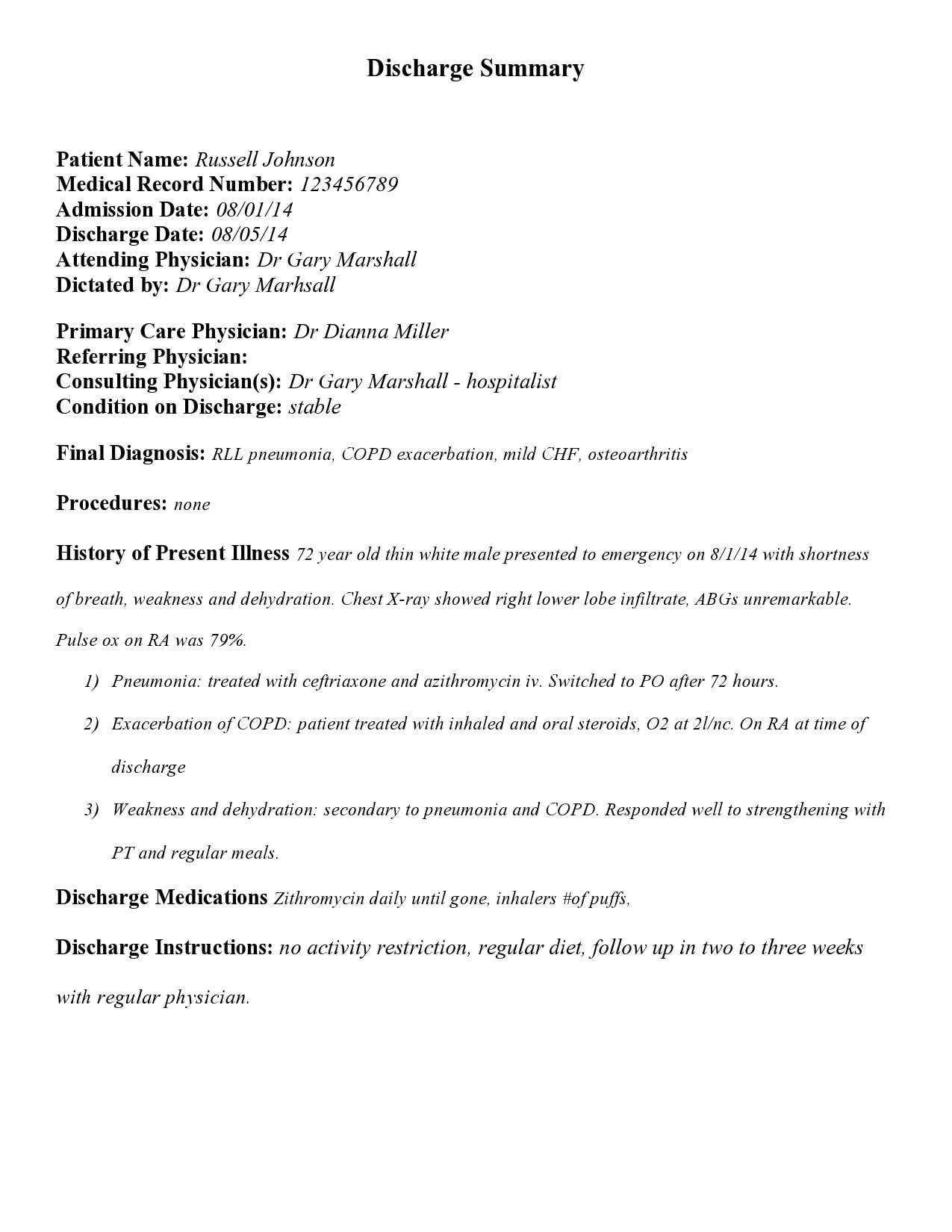
In general, this document is the main mode of communication between the healthcare team of the hospital and the providers of aftercare. A discharge summary example is an official document and as such, might jeopardize the care if the doctor makes any errors while making it. These are the steps that doctors follow when completing a discharge summary:
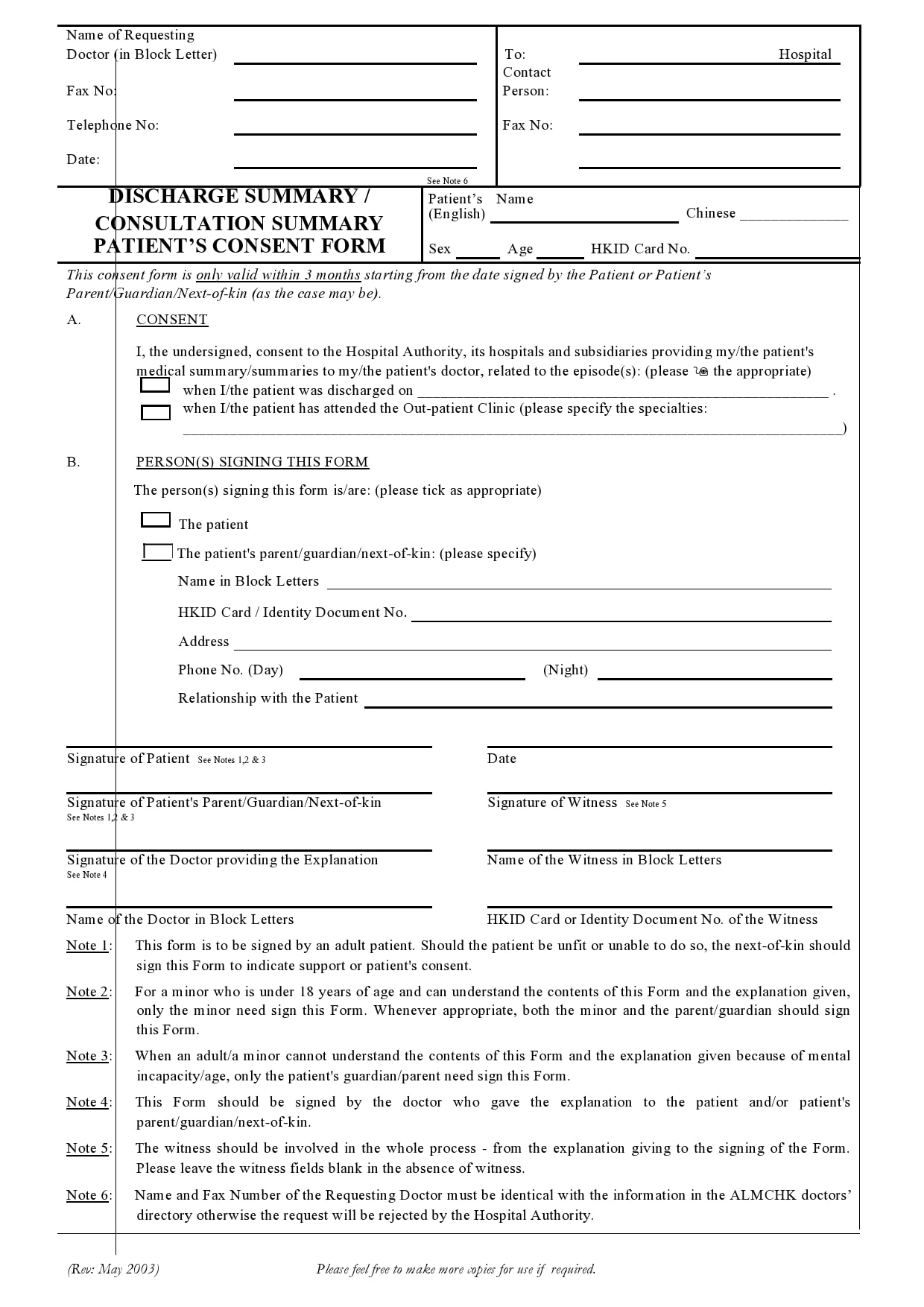
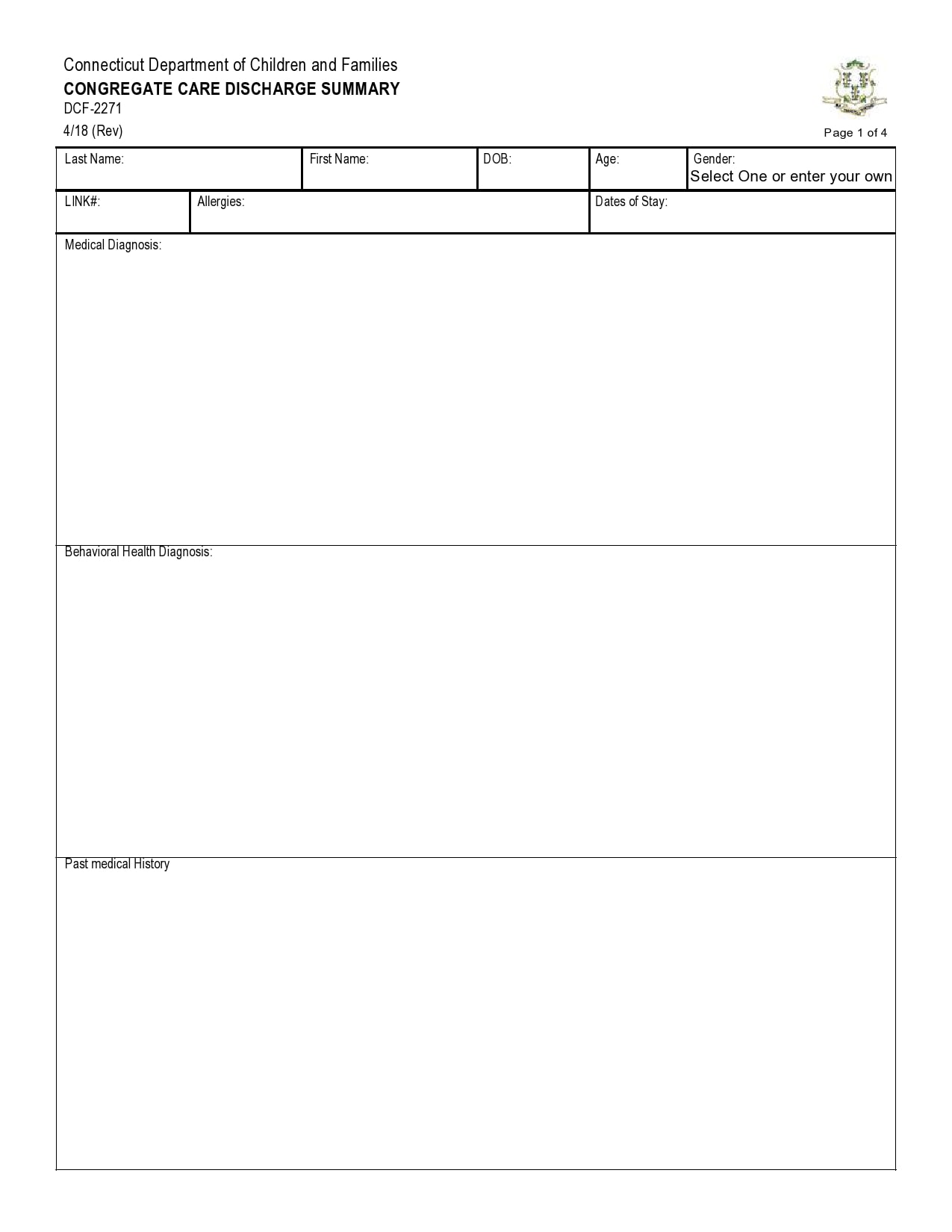
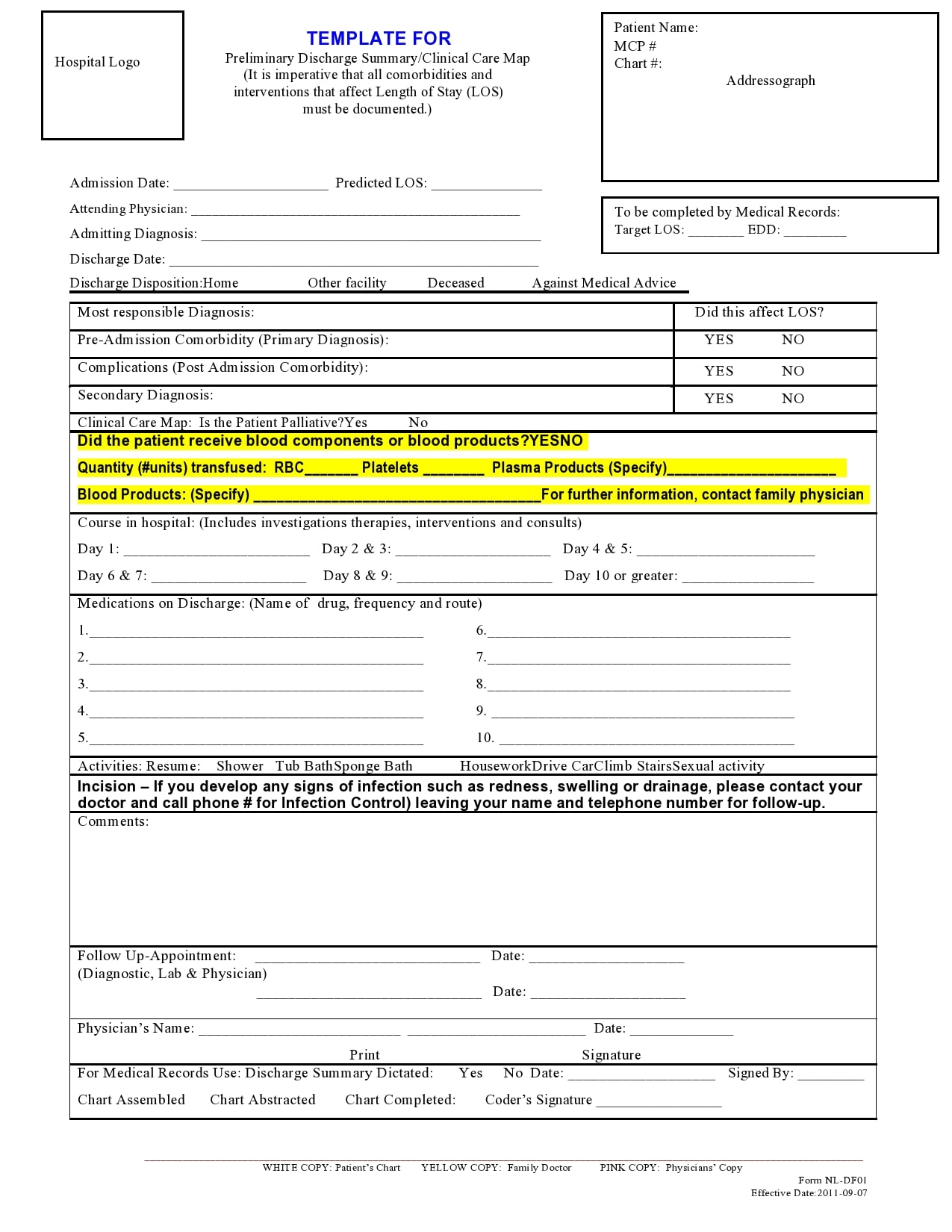
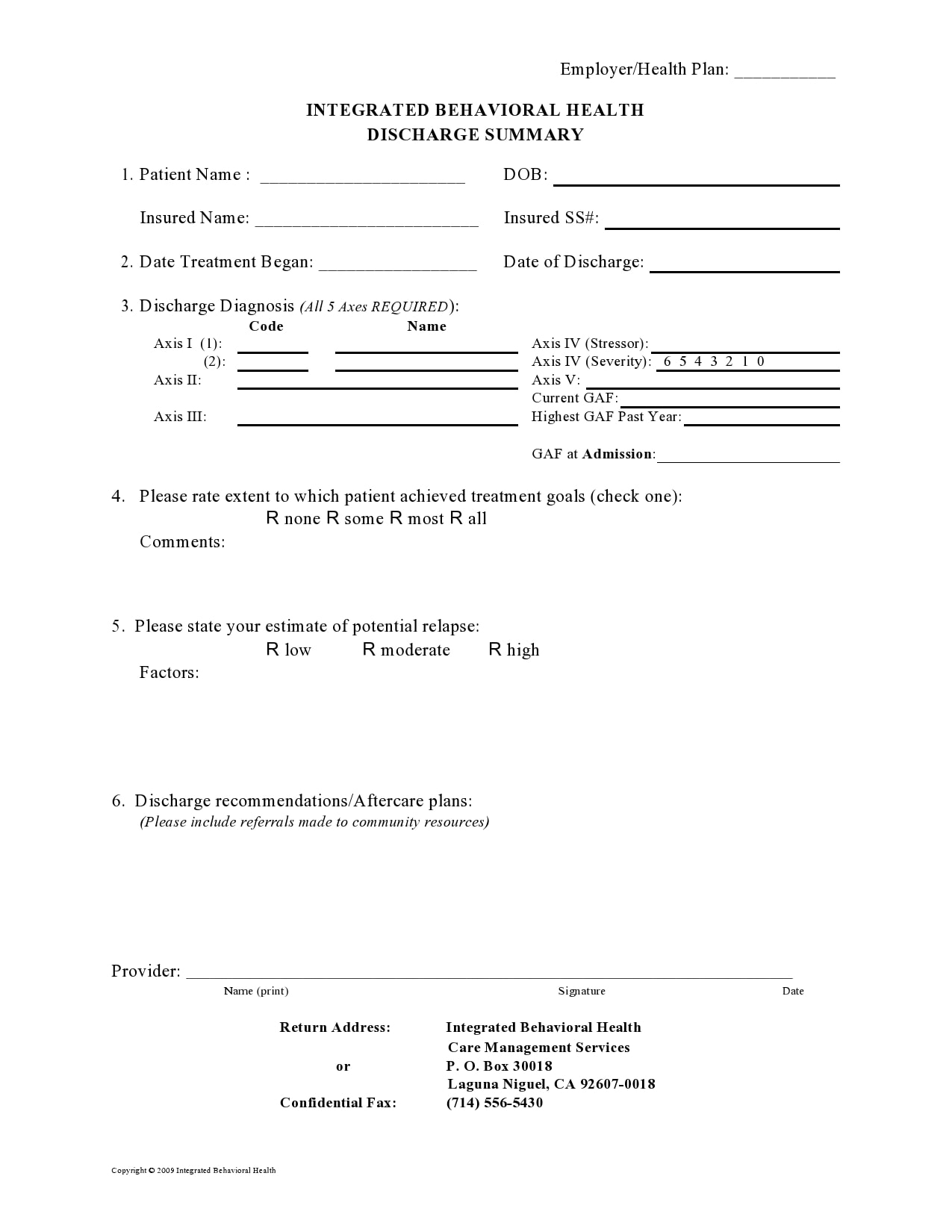
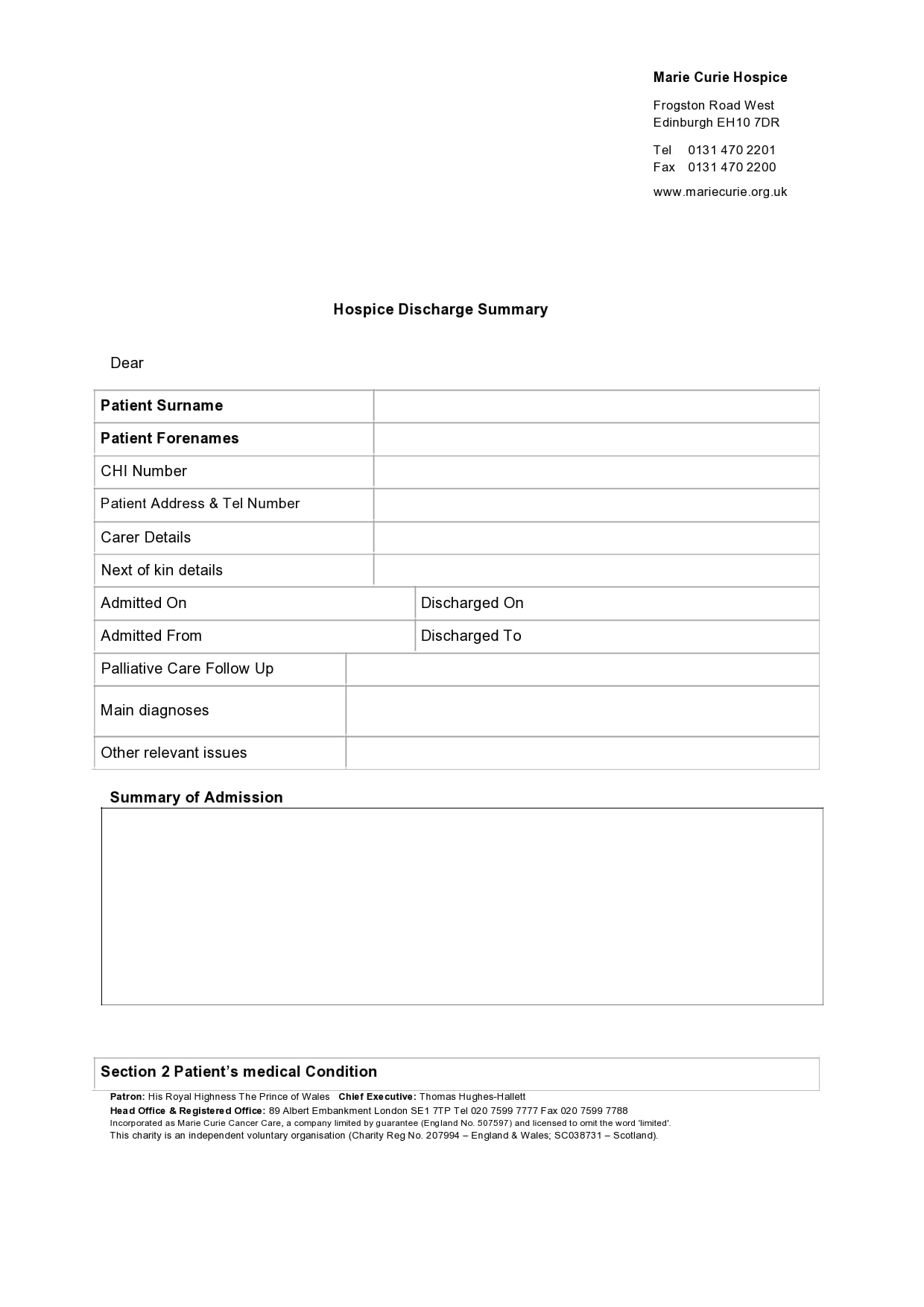
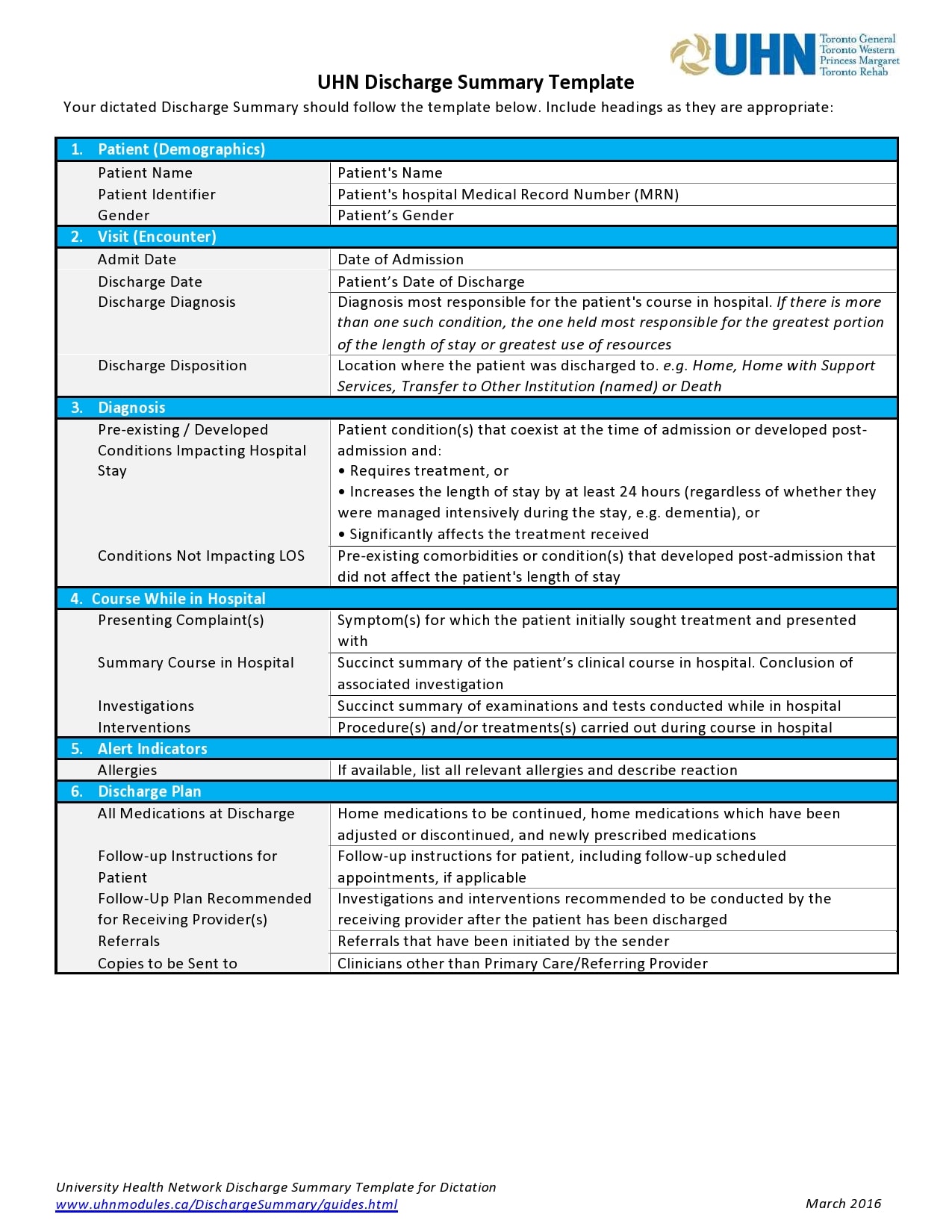
- The patient’s details
These include the following:
The complete name of the patient.
The patient’s date of birth.
An identification number (each patient gets a unique ID number).
The complete address of the patient.
The telephone number of the patient.
The sex of the patient at birth.
The gender that the patient identifies with (this may vary with their sex at birth).
The ethnicity of the patient.
The patient’s emergency contact or next of kin and the relevant details. - Details of the general practitioner
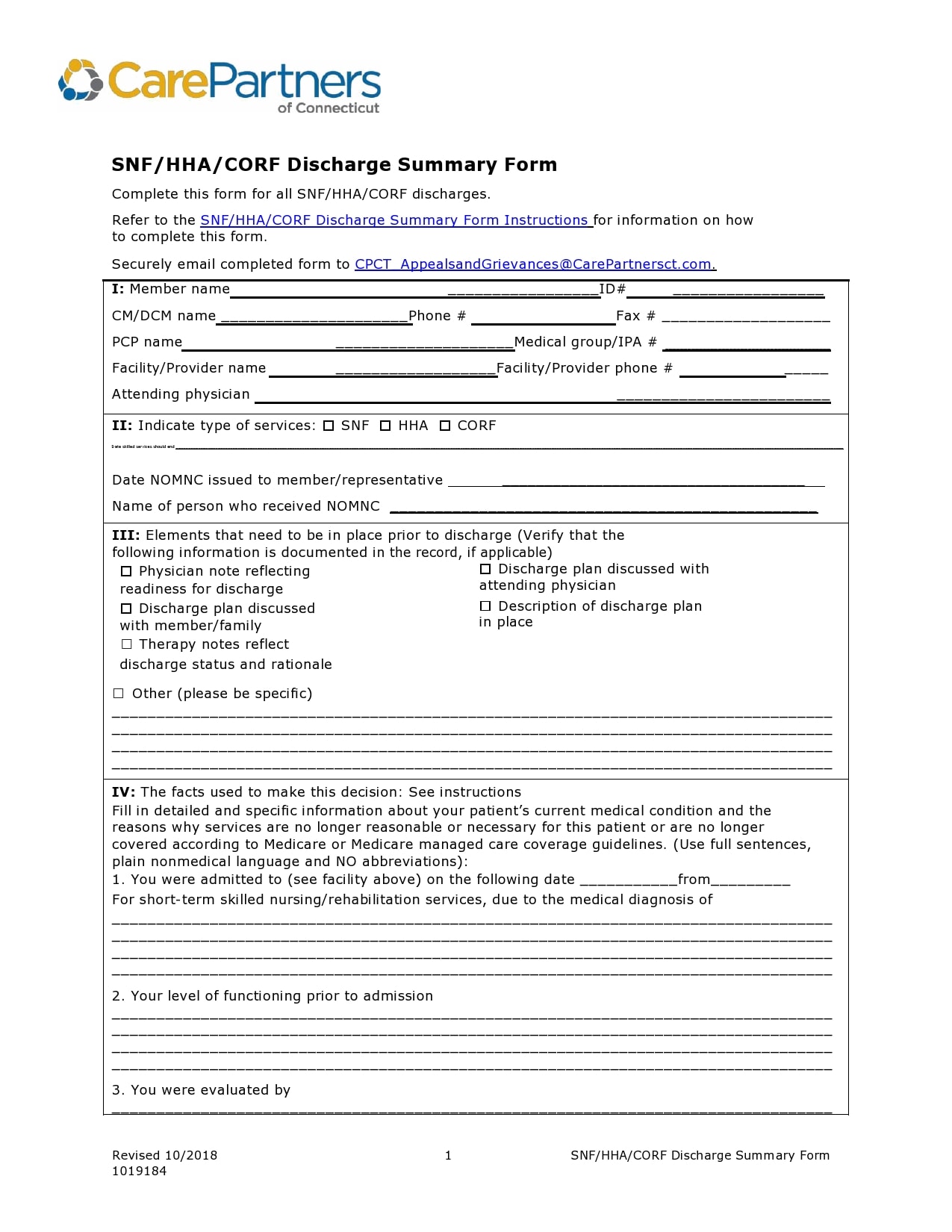
This part of the summary contains the details of the GP in charge of the patient. - Details about the hospital
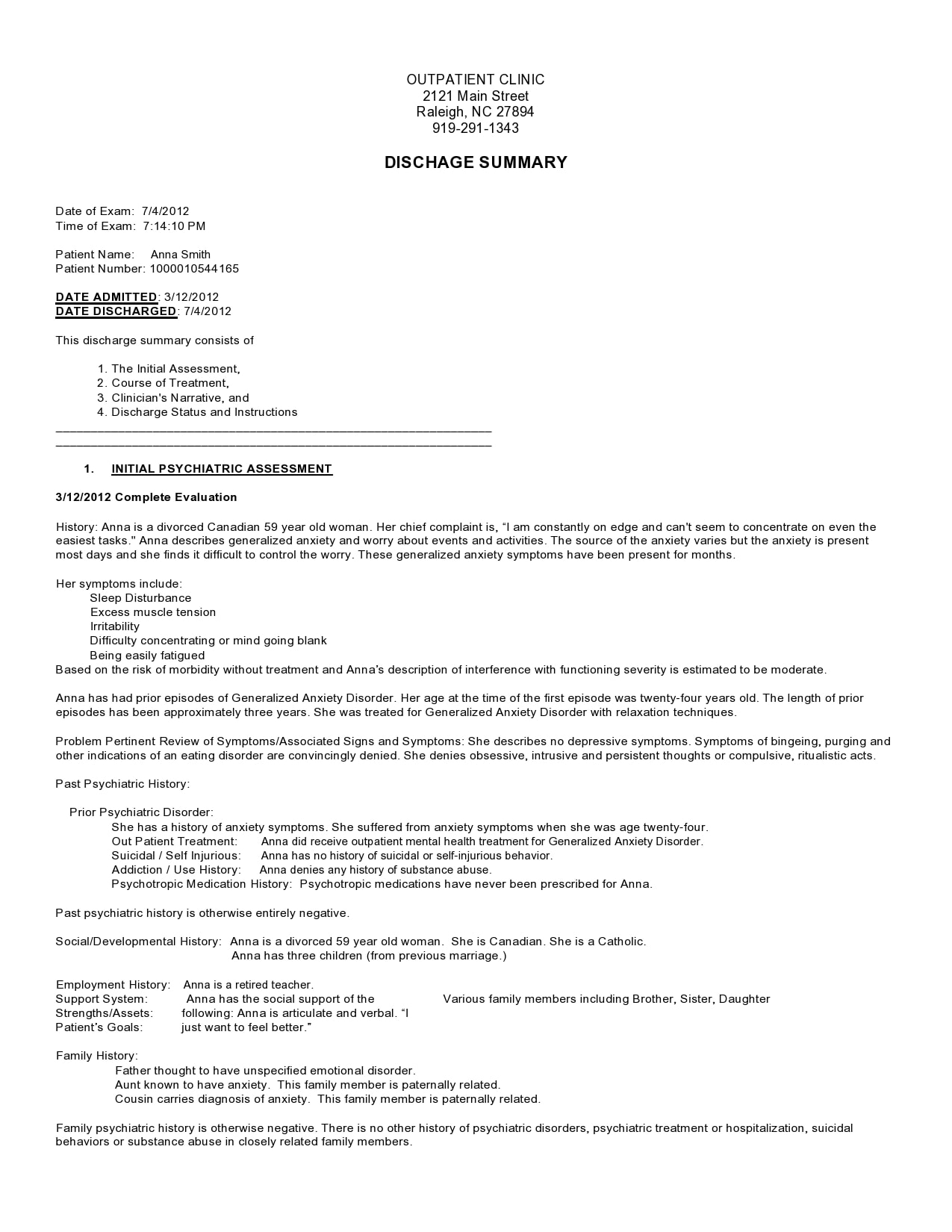
This section includes the important aspects of the discharge of the patient. - History and findings of examinations
This section includes a comprehensive summary of the presenting signs and symptoms of the patient. - Diagnoses
Included in this section is the diagnosis or diagnoses made during the patient’s stay in the hospital. If there is no confirmed diagnosis, use the main complaint and give an explanation of why the doctor didn’t identify any cause. It’s important to be very specific when documenting this information. - Management
This section provides an explanation of how the healthcare team managed the patient during their stay in the hospital. It may include any initiated long-term management processes. - Complications
This section includes any complications that may have occurred during the patient’s stay in the hospital. - Procedures
This section document all of the procedures and operations that the patient went through. - Future management
This section includes the details of the plan to manage the patient and their conditions after getting discharged from the hospital. Any actions that the GP of the patient needs to do after discharge must be clearly documented. - Changes in medication
A short summary of any changes to the regular medications of the patient explanations for the changes. - Medications for the patient to bring home
A list of all the medications that the patient is currently on along with the details for taking them. - Adverse reactions and allergies
This section provides an outline of any adverse reactions or allergies that the patient experienced. - Instructions for the patient
This section summarizes the key information regarding the patient’s stay in the hospital. It is usually written in a patient-friendly language to make it easy to understand. - The person who wrote the summary
This section contains personal information regarding the healthcare provider who completed the document.

")
