
As a nurse, you are one of the front liners in medical emergencies. In the course of your duties, you take notes on every interaction you have with patients. These notes are very important as you are usually the one who administers drugs to patients in the hospital. You need to know how to write nursing note samples that you can use as needed.
Contents
Nursing Note Samples
What is a progress note in nursing?
Generally speaking, nurses are patient advocates for the simple reason that you often spend the most time with patients. Creating nursing note samples provides you with the complete picture of patient’s health that other medical specialists and professionals can use in making diagnoses or suggesting treatments.
These notes are a form of official documentation made by nurses when charting patients. On your nurses’ notes templates, you jot down important information based on the scribblings and notations you gather during your visits with the patients.
You may also incorporate charting by exception. This is a shorthand way of jotting down the “exceptions,” – the abnormalities a patient experiences by initialing charts and lists. Keeping accurate and thorough notes is extremely essential in the maintenance of effective communication between you and the rest of the medical staff.
If you consider the number of patients that you attend to at any given time, the notes you take will help you better remember the events that transpired throughout the day, the care you provided, and the specialists involved with each of the doctors and medical professionals.
The benefits of writing nursing notes
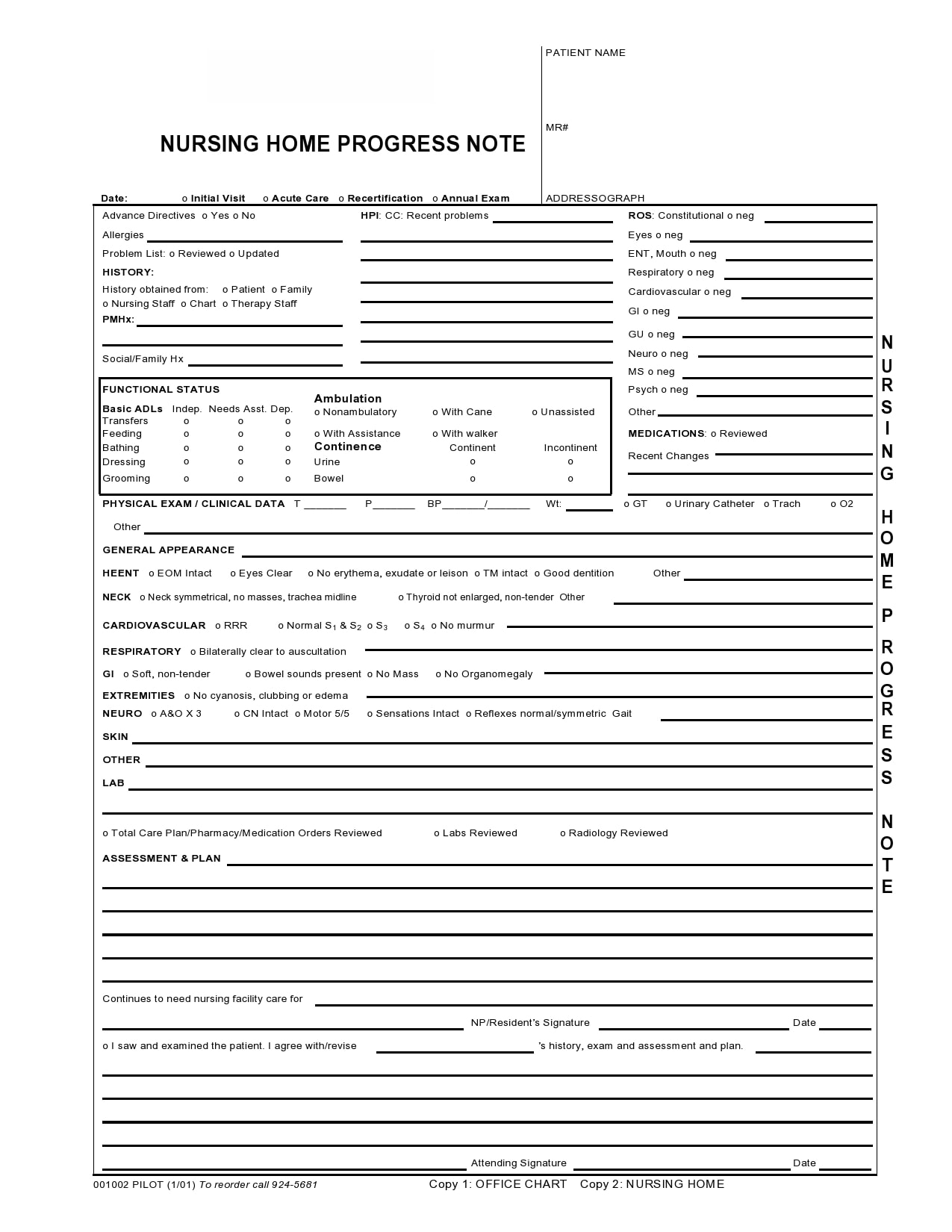
Typically, nursing note samples carry a patient’s general and basic information. It may include the following:
- The appearance of the patient
- Medical history of the patient
- Current medical condition of the patient
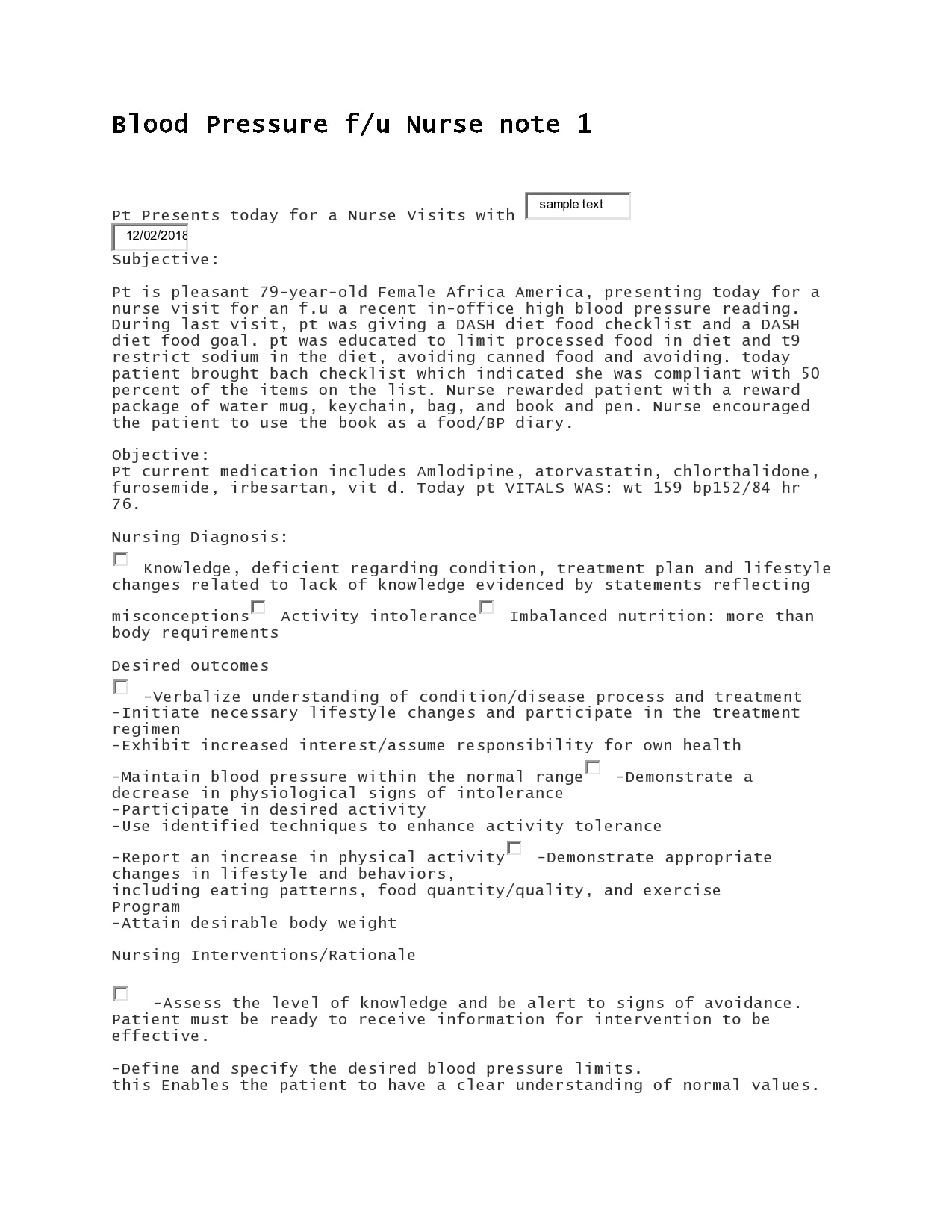
It could also contain information about a specific person including your observations and your opinions based on those observations. For instance, many nurses create nursing progress notes examples after conducting nursing assessments and tests.
Fundamentally, these notes provide information relevant to a patient’s overall medical status. The notes can primarily help you keep a record of your observations about patients. As a part of your work, there is a need to include in your notes the behaviors and activities of your patient – both unusual and usual – as observed.
The information provided by your notes can help you monitor any changes in a patient’s behavior and condition over a specific period of time. This consequently, can help you determine what causes these changes.
You may also use a blank note as a reminder to yourself, another nurse or some other medical professional attending to the condition of the patient. This avoids confusing the conditions of the patients in the hospital.
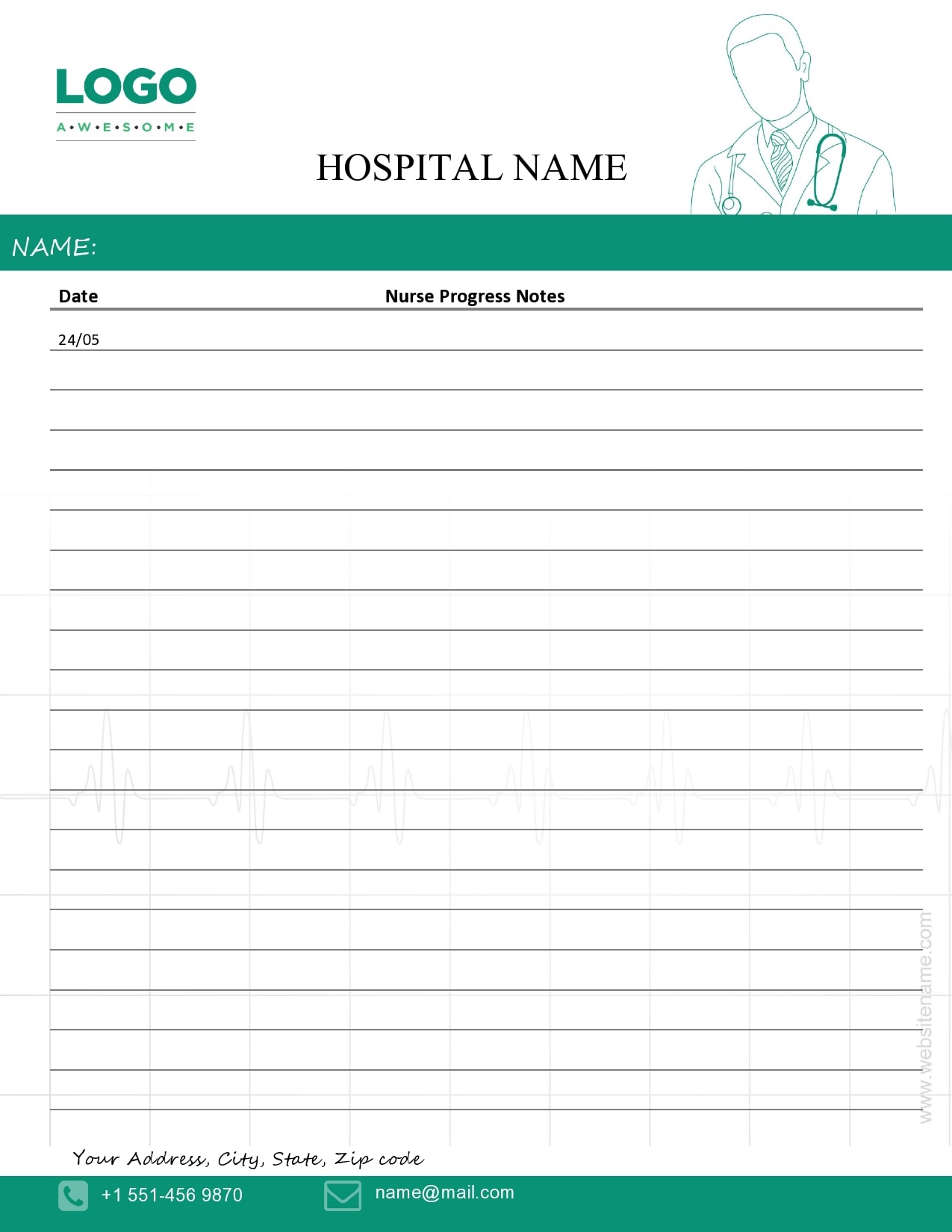
Nurses Notes Templates

What to include?
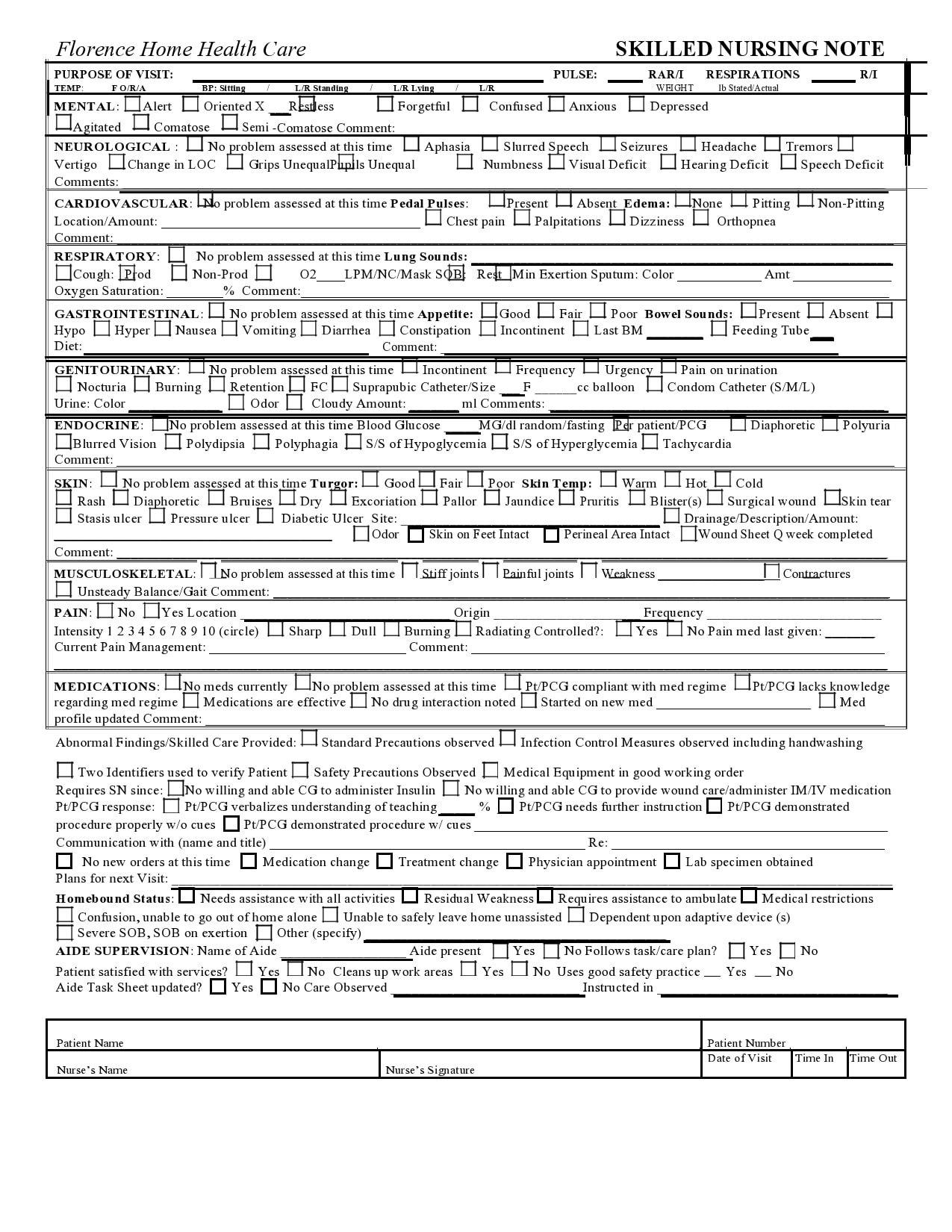
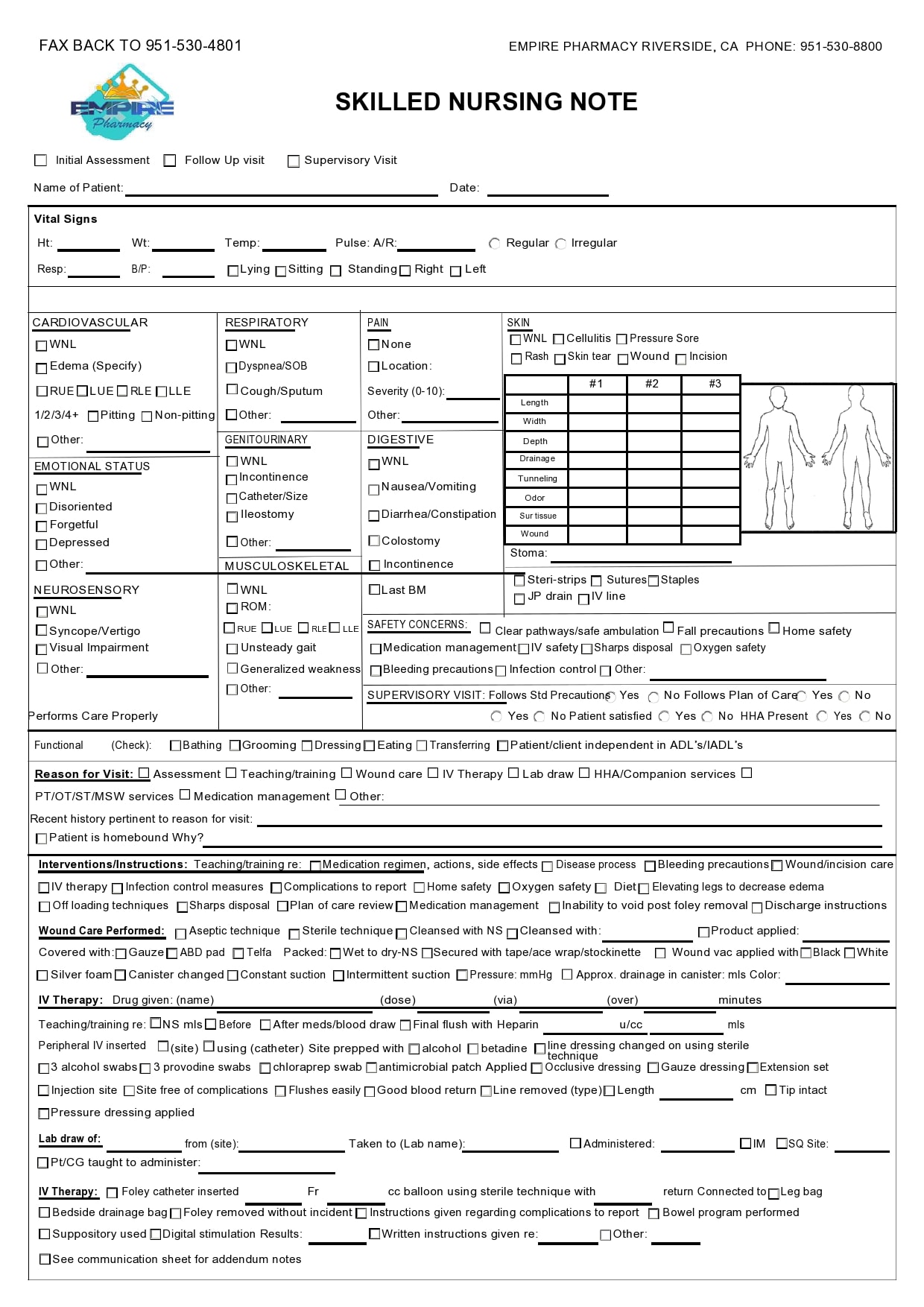
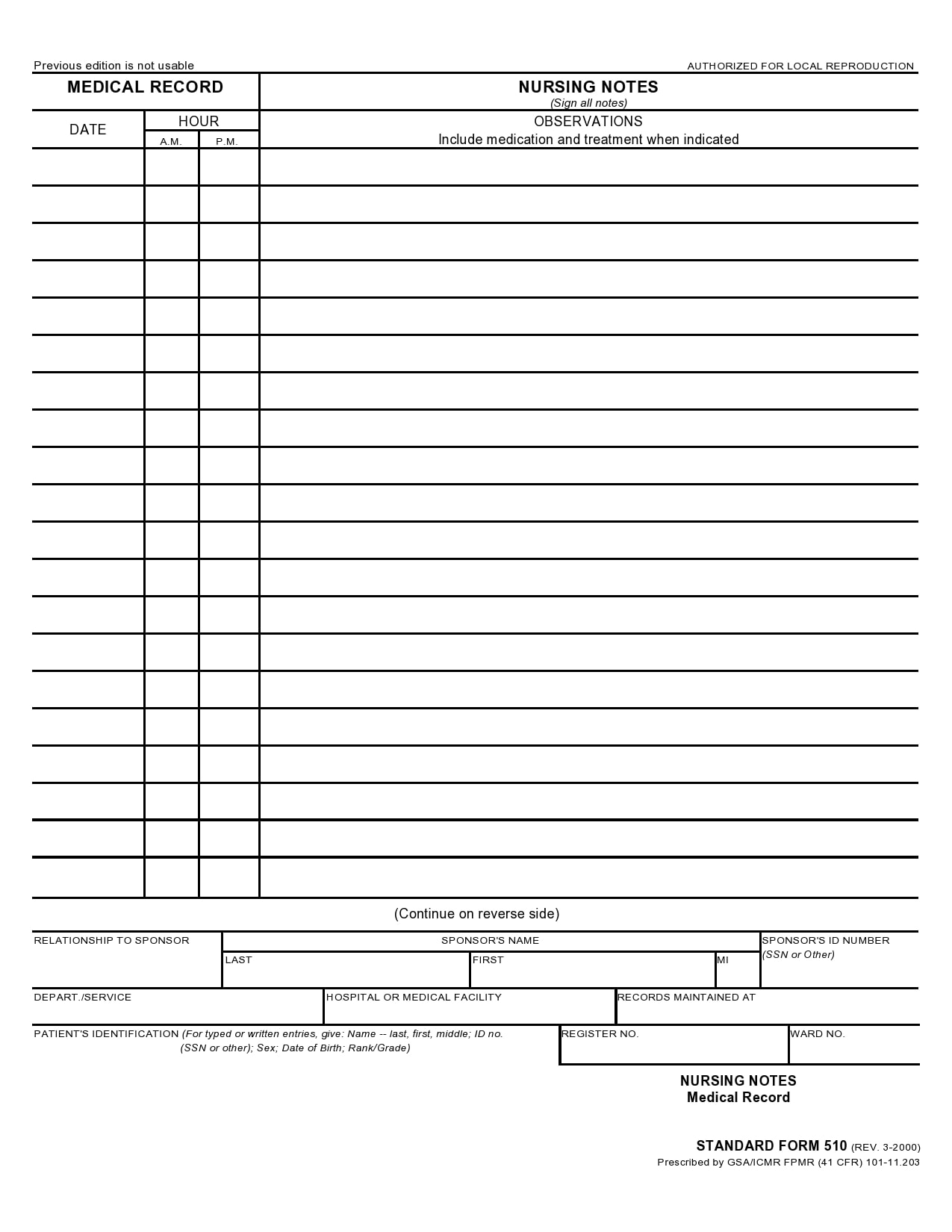
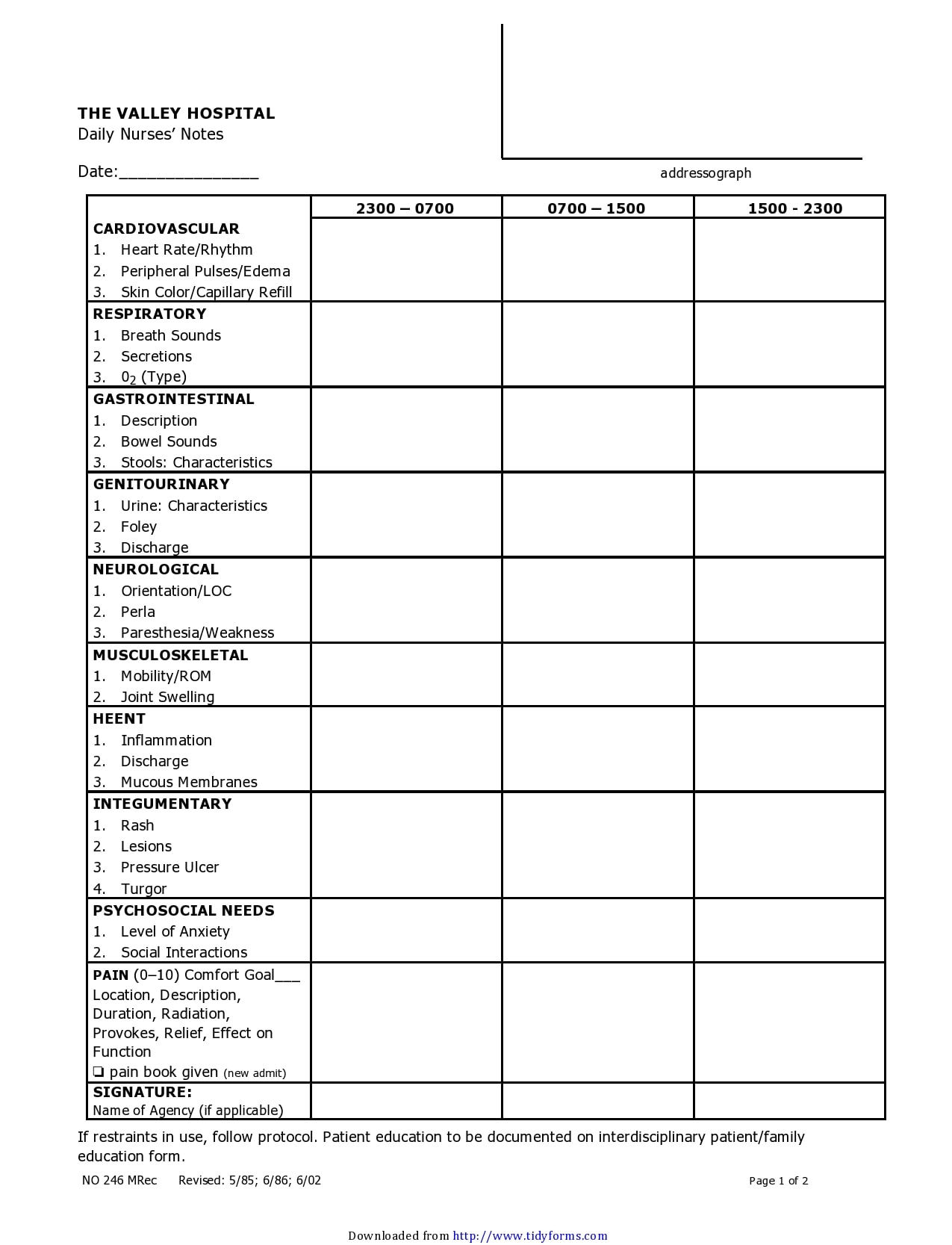
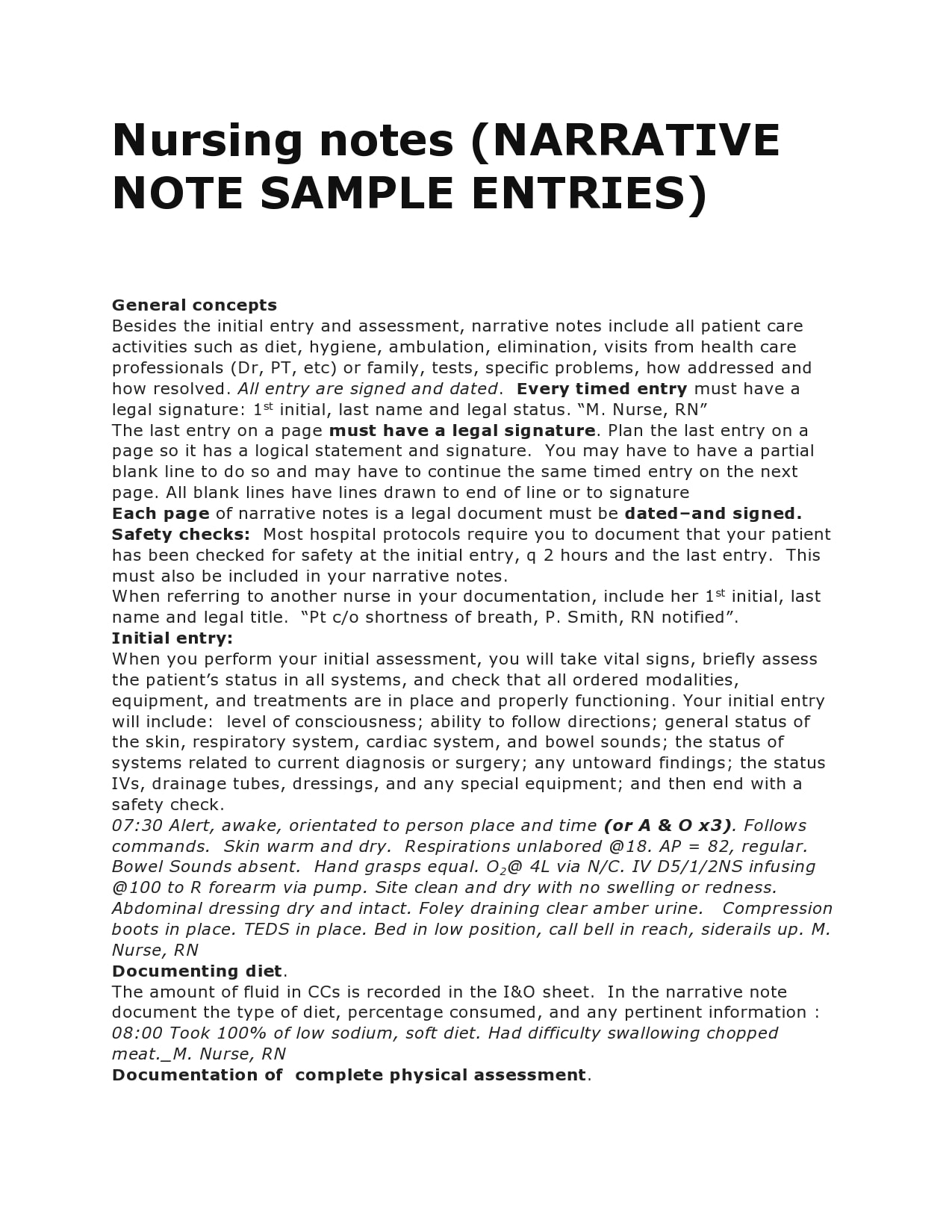
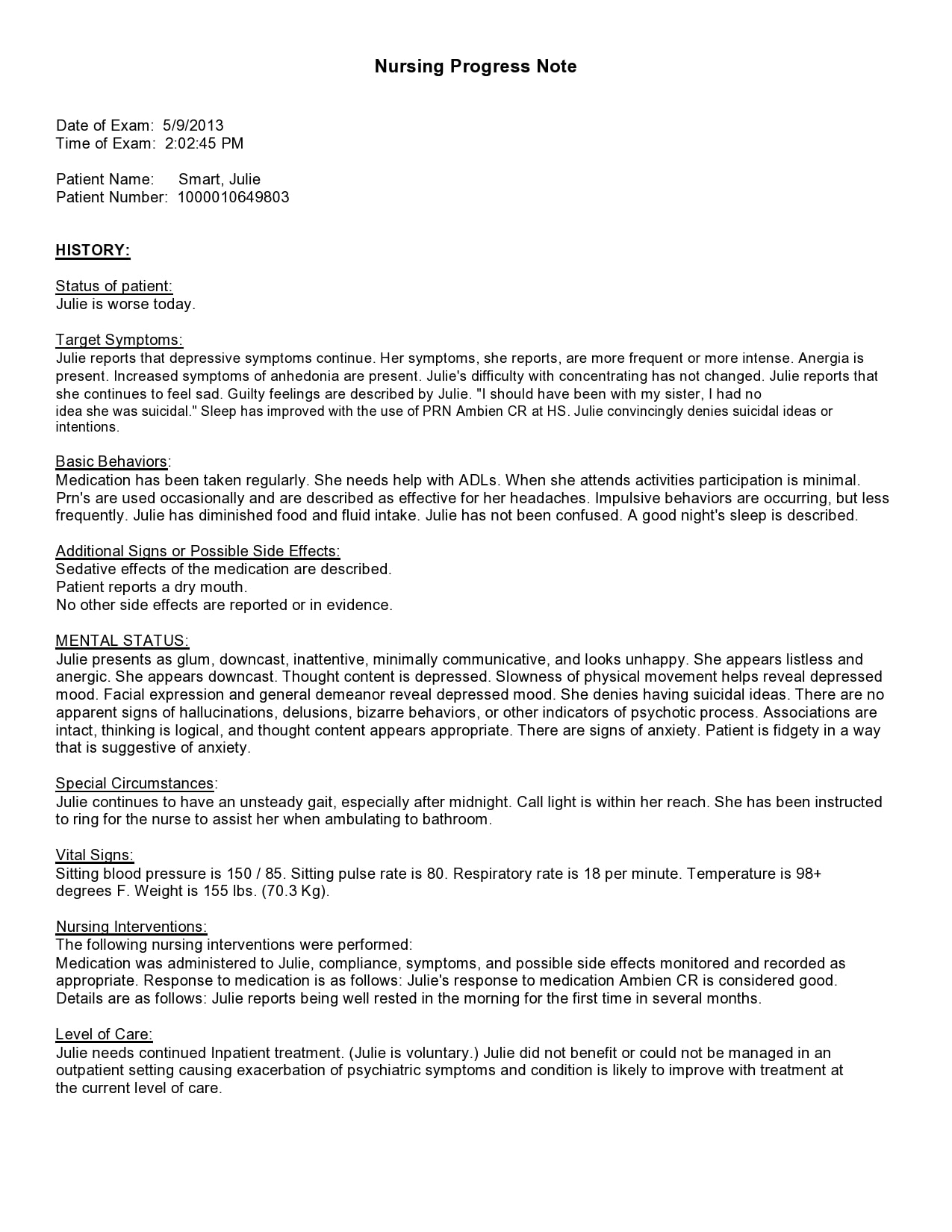
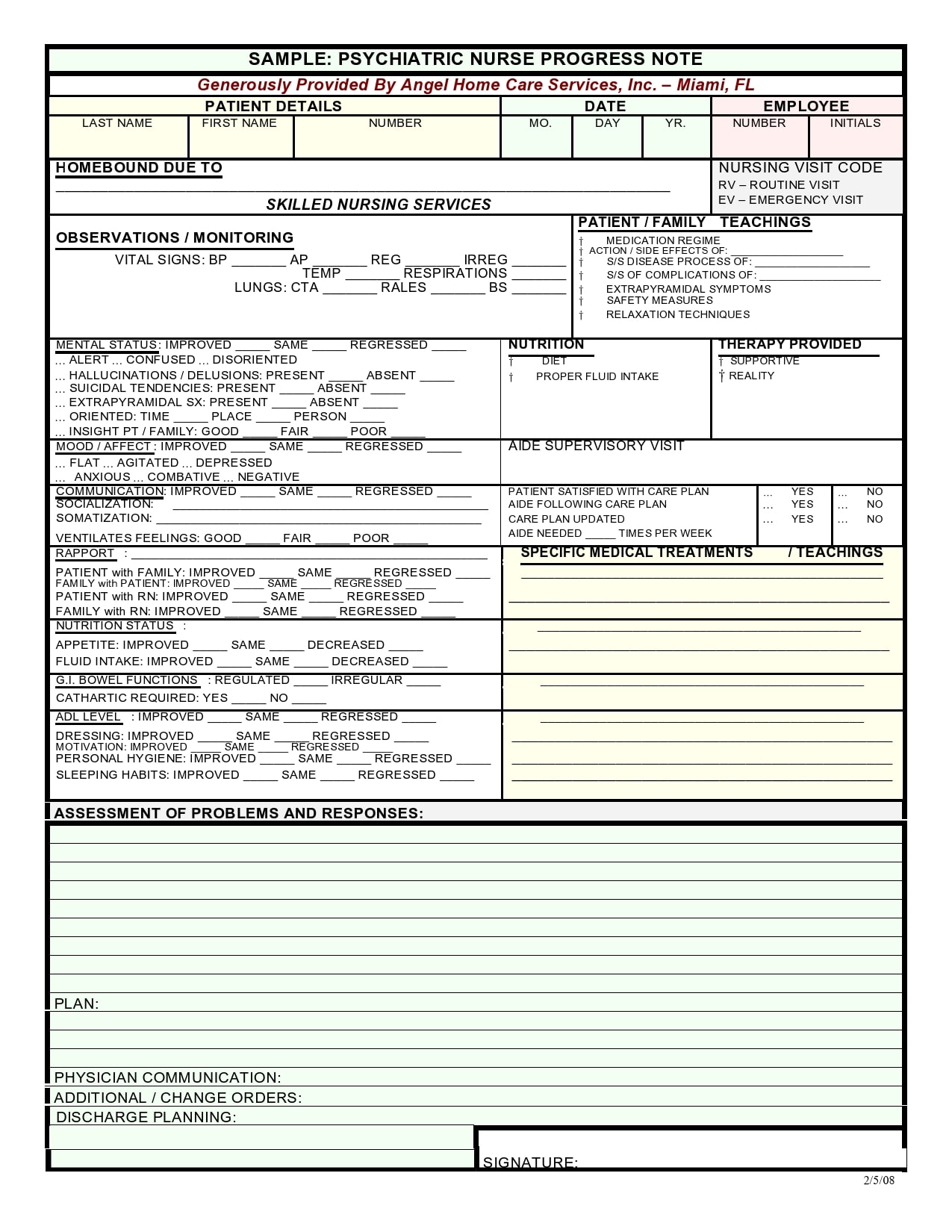
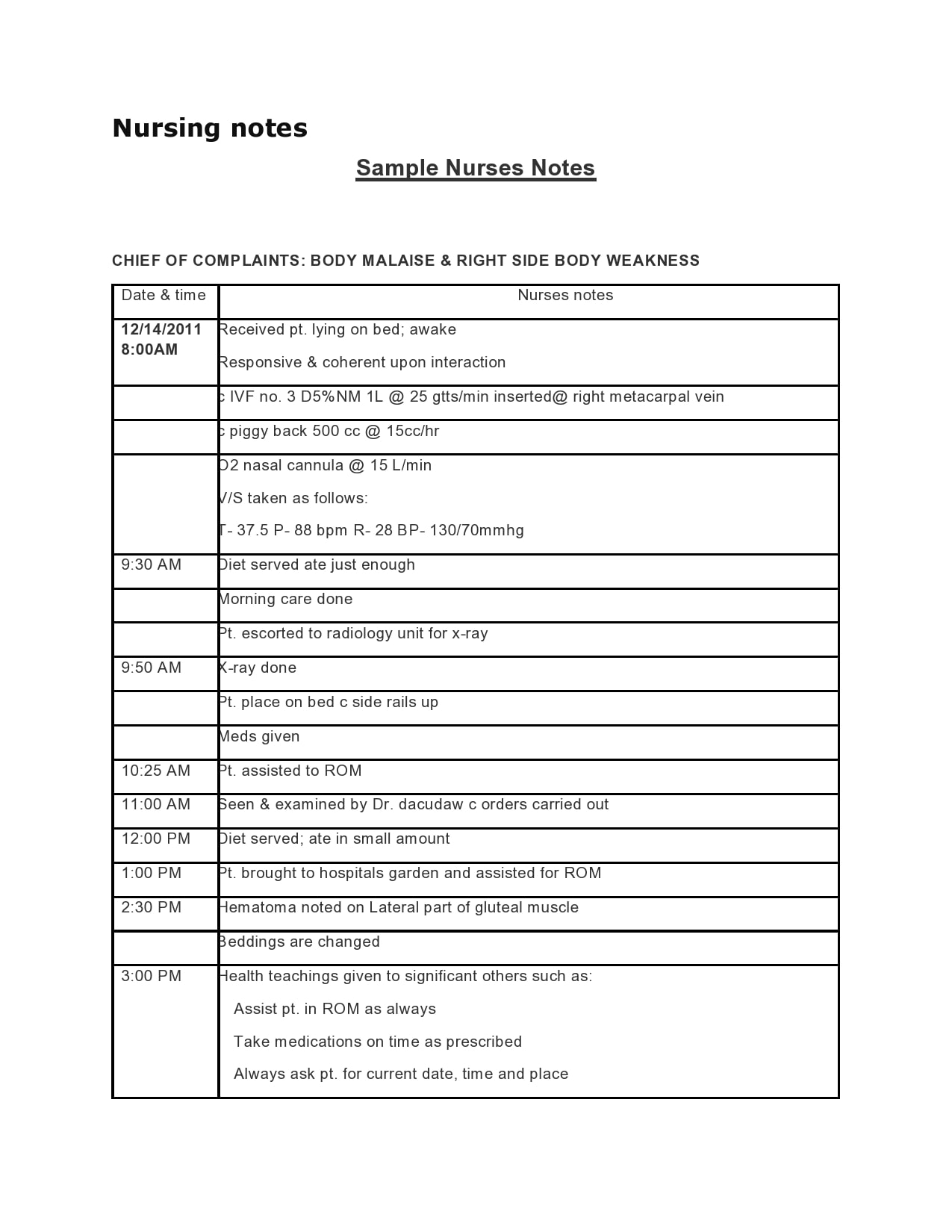
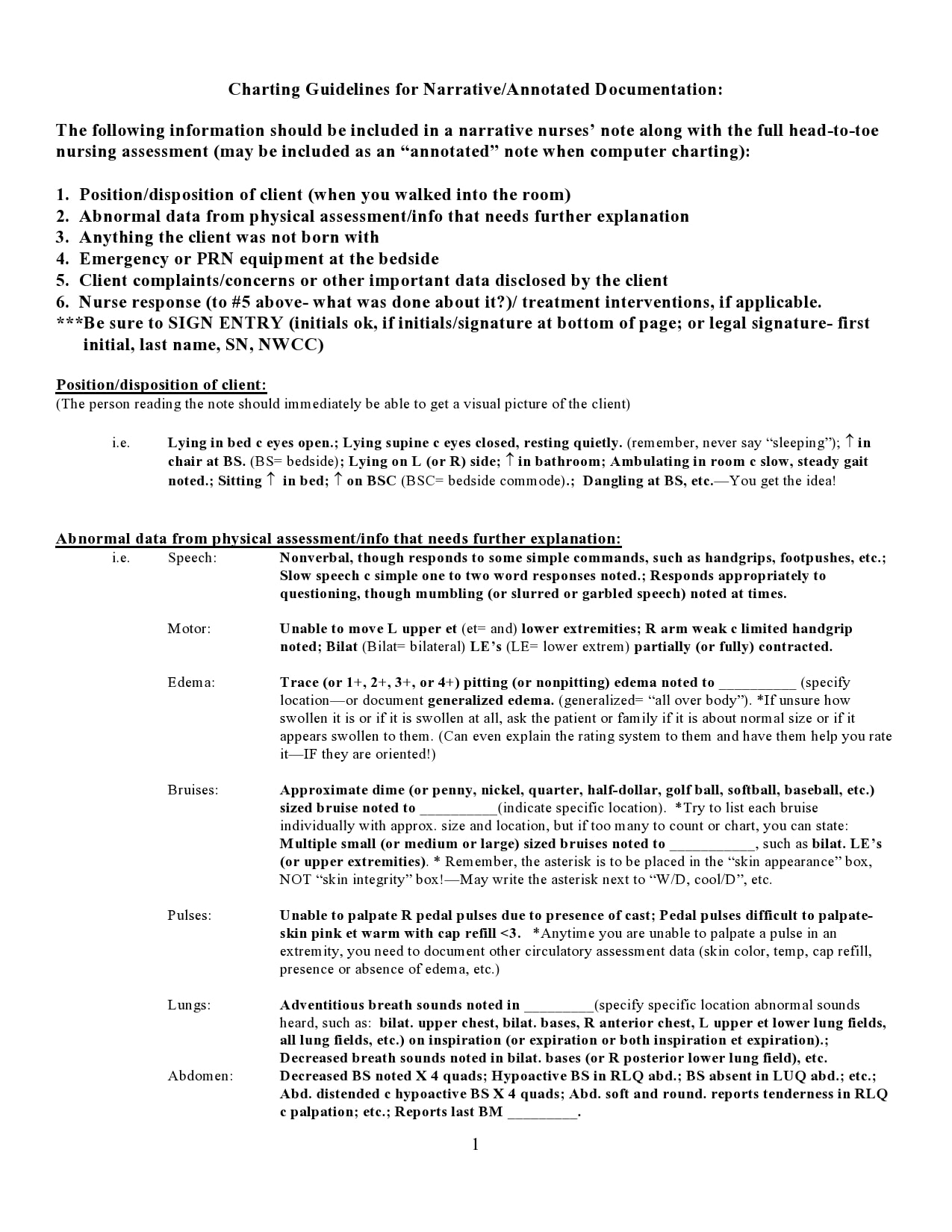
Nursing note samples contain pages with lines and a title that says, “Progress Notes” or “Nursing Notes.” But there is a lot more to these notes. For one, you should consider the pages as legal documents and as such, they carry some degree of significance. This document includes the following:
- The time and date
- The name of the patient
- Your name as the attending nurse
- The reason for the patient’s visit
- The patient’s appearance
- The vital signs of the patient
- Your initial assessment of the patient
- Any diagnostics or labs requested
- An evaluation of any medical interventions conducted
- Any significant instructions given
- Any family interactions that the patient had
- Observations and recommendations
- Anything unusual that you have observed
The most important information to document
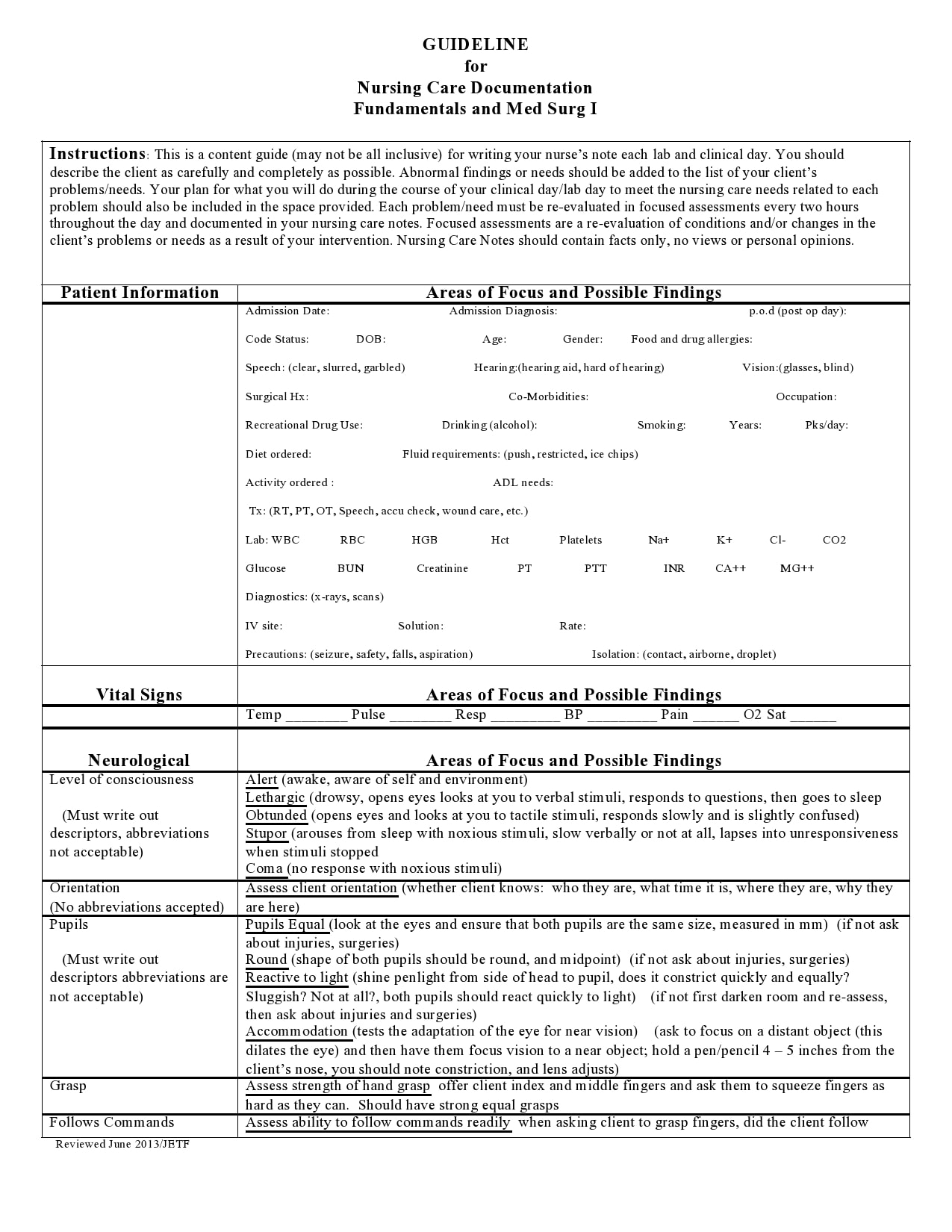
As a nurse, you can discern in your observations what you must write down in your nursing note samples. This is a very important aspect of the use of the notes. But more important is to understand who you’re writing for, as well as, when and why you need to write them.
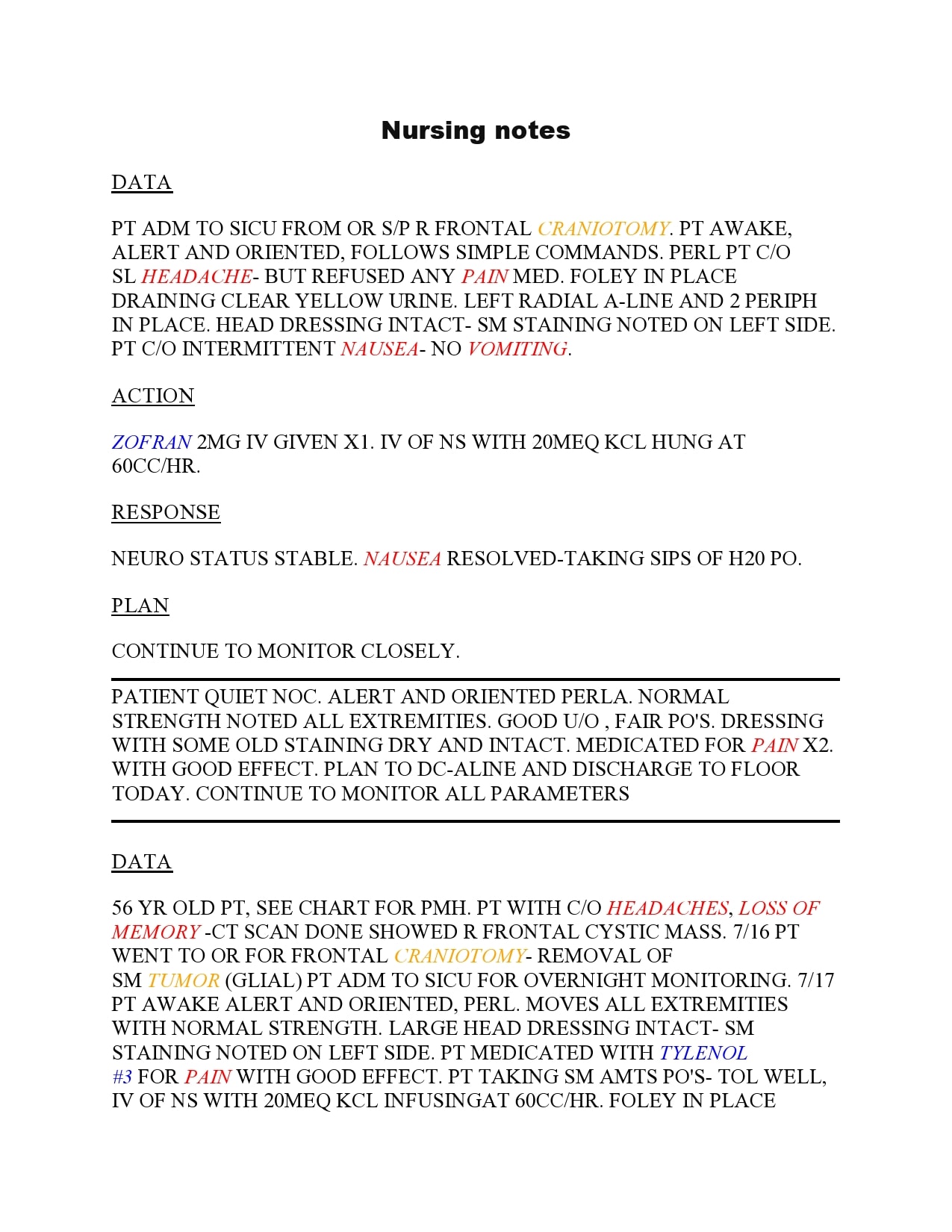
There is, therefore, a need to understand the basics of skilled nursing documentation templates. There are three issues that you must address each time you write these notes:
- Description
You should describe what’s going on with your patient. Describe the patient’s condition. Include what you see, hear, smell, felt, and so on. Also, include the remarks of the doctor if deemed necessary. - Action
Describe the actions that you or the doctor have taken in response to the patient’s condition. Typically, this may include giving medication, ensuring the patient’s safety, and the like. - Response
Give a description of how the patient responded to the actions taken. This determines whether the patient improves because of your actions or your actions have no effect and you need to try something else.
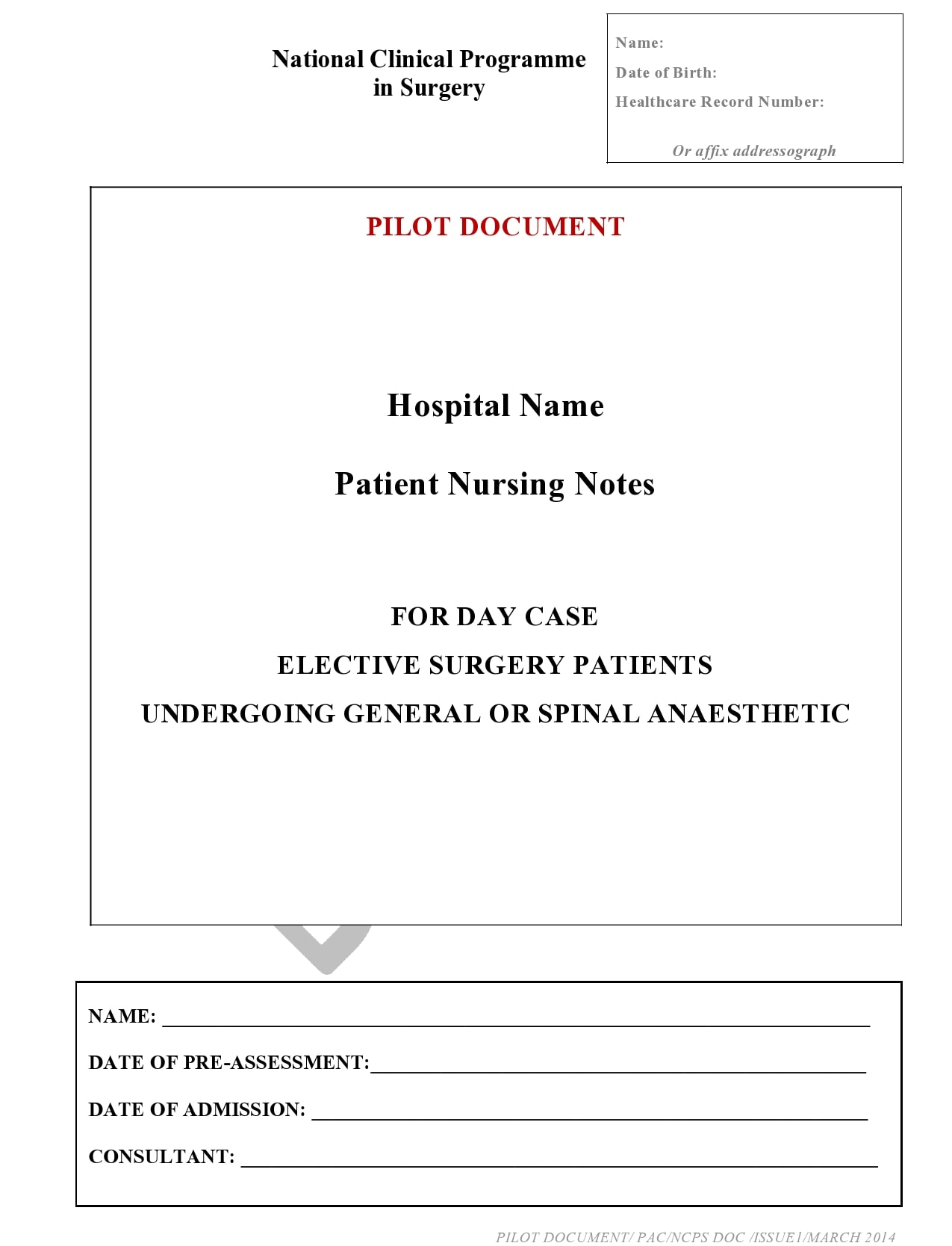
Nursing Notes Examples
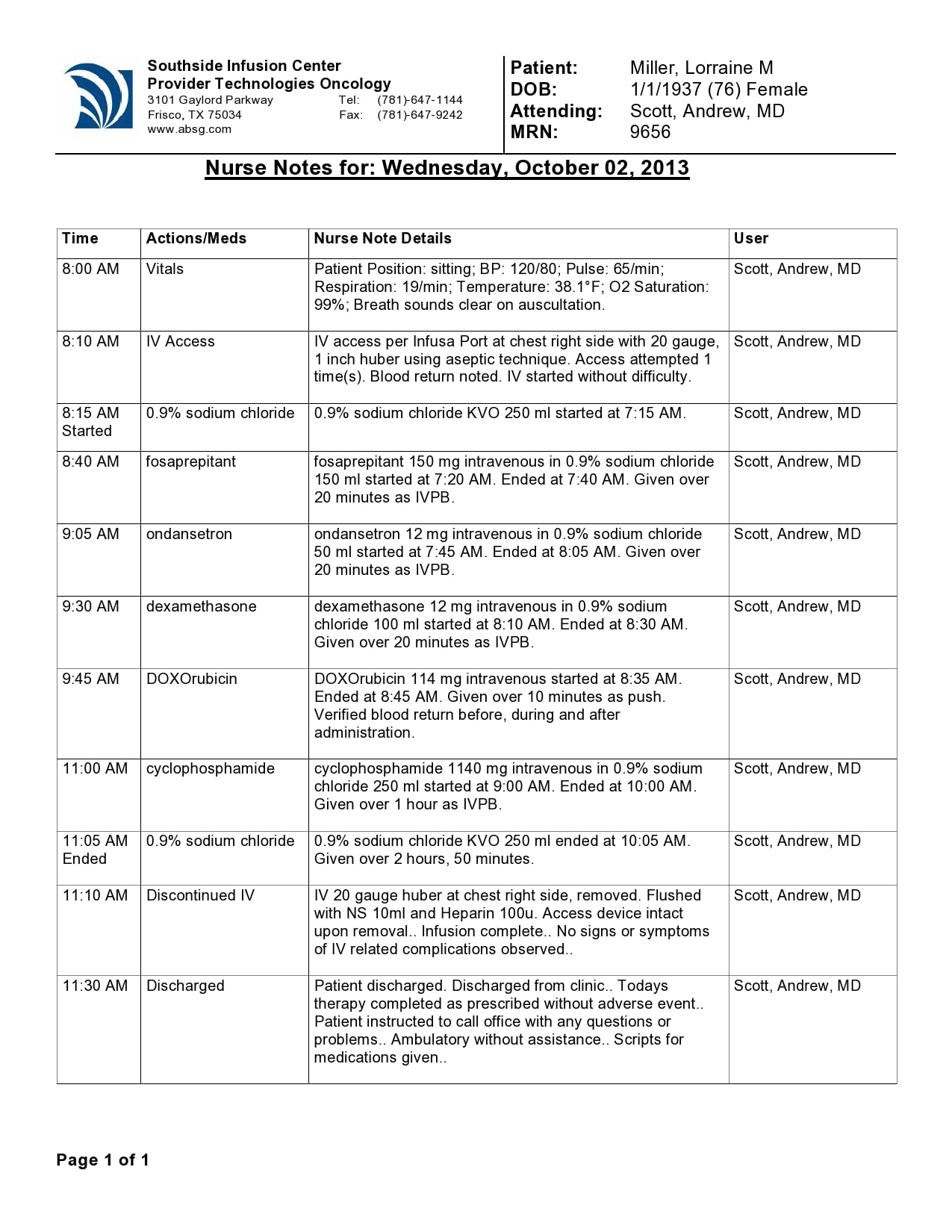
How do you write a nursing note?
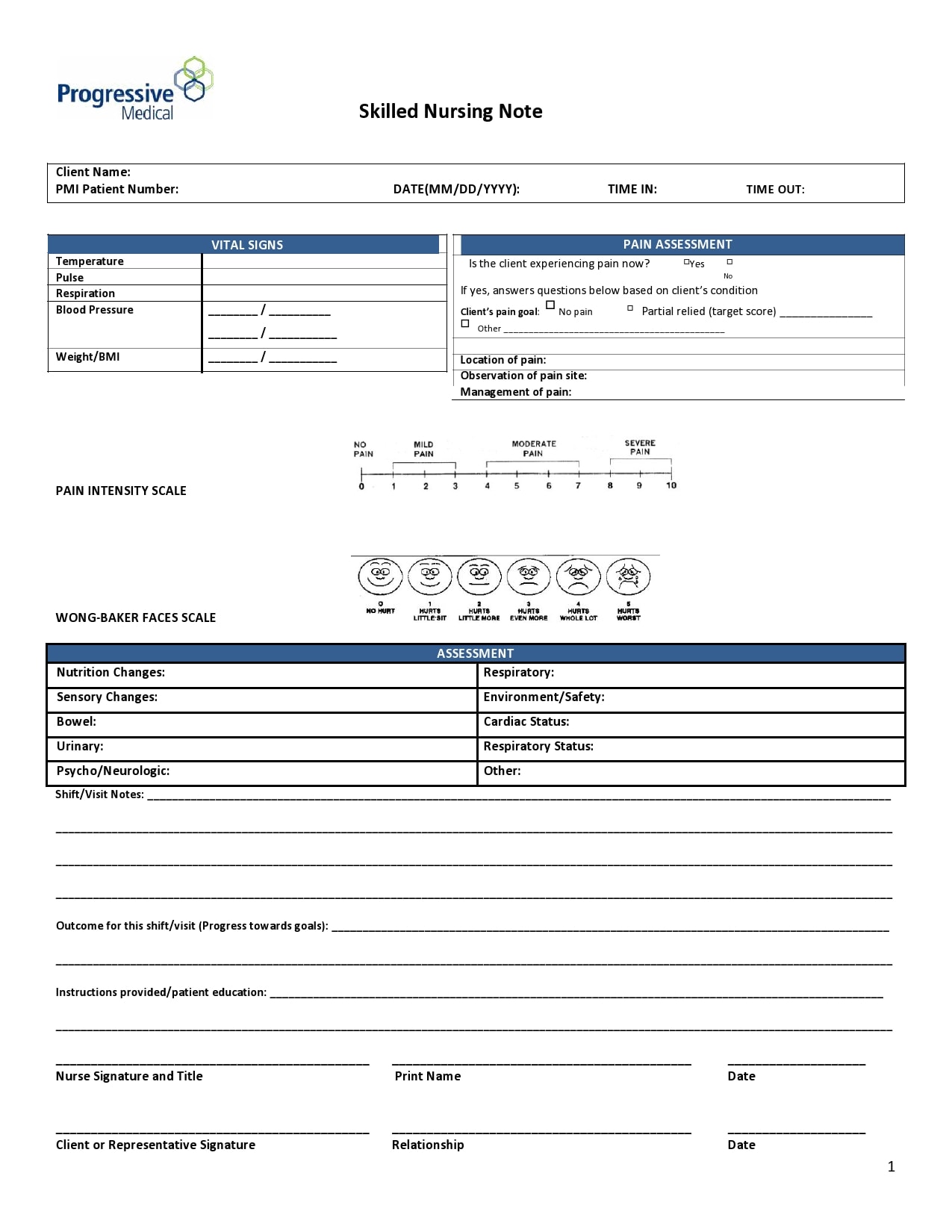
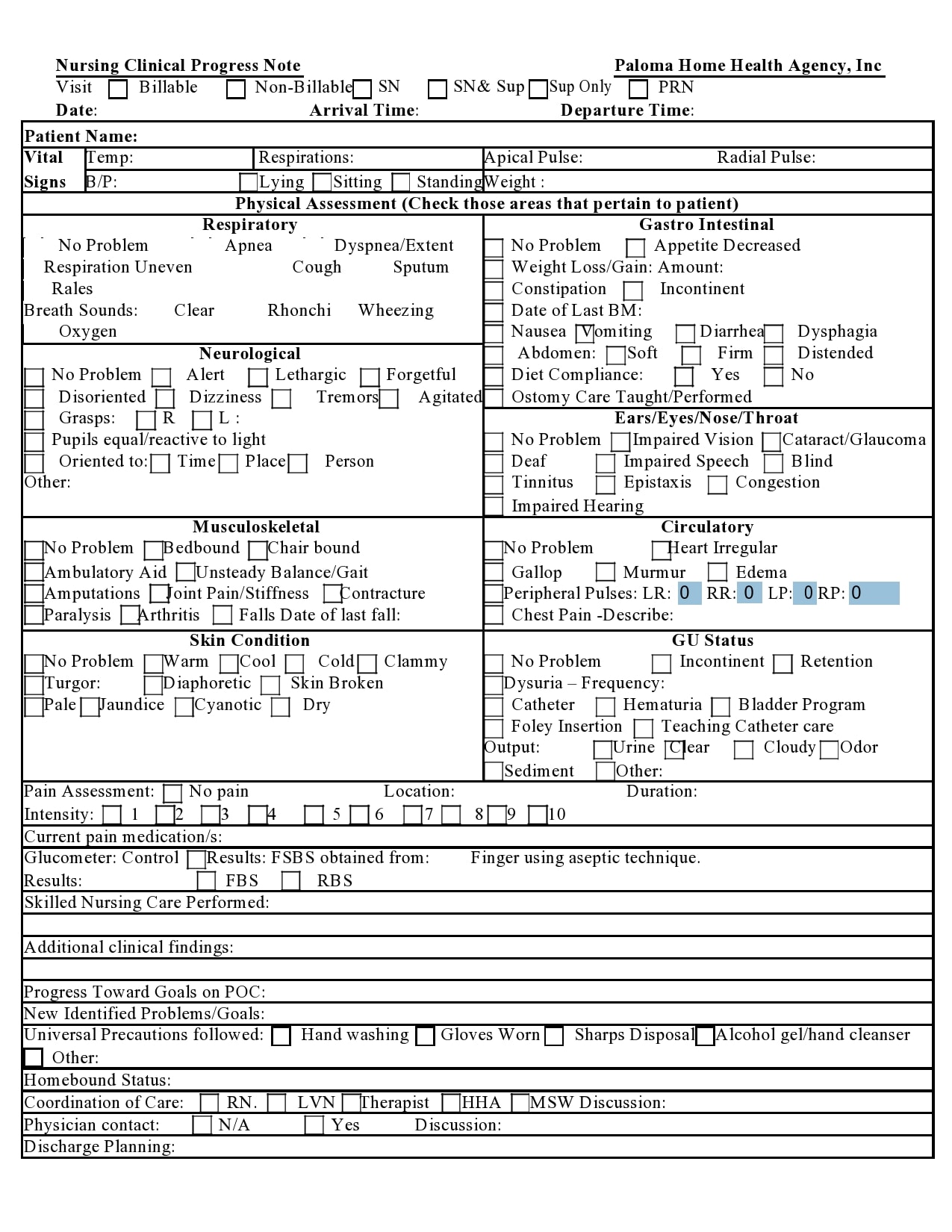
Nursing notes are health or medical records written by a nurse. Most nurses notes templates include the following:
- Accurate nursing assessments or documentation
- Observed changes in the condition of a patient
- Care or treatment given to the patient
- Other relevant information to support the clinical team
If you want to make the most effective notes, consider these tips taken from the best nursing progress notes examples:
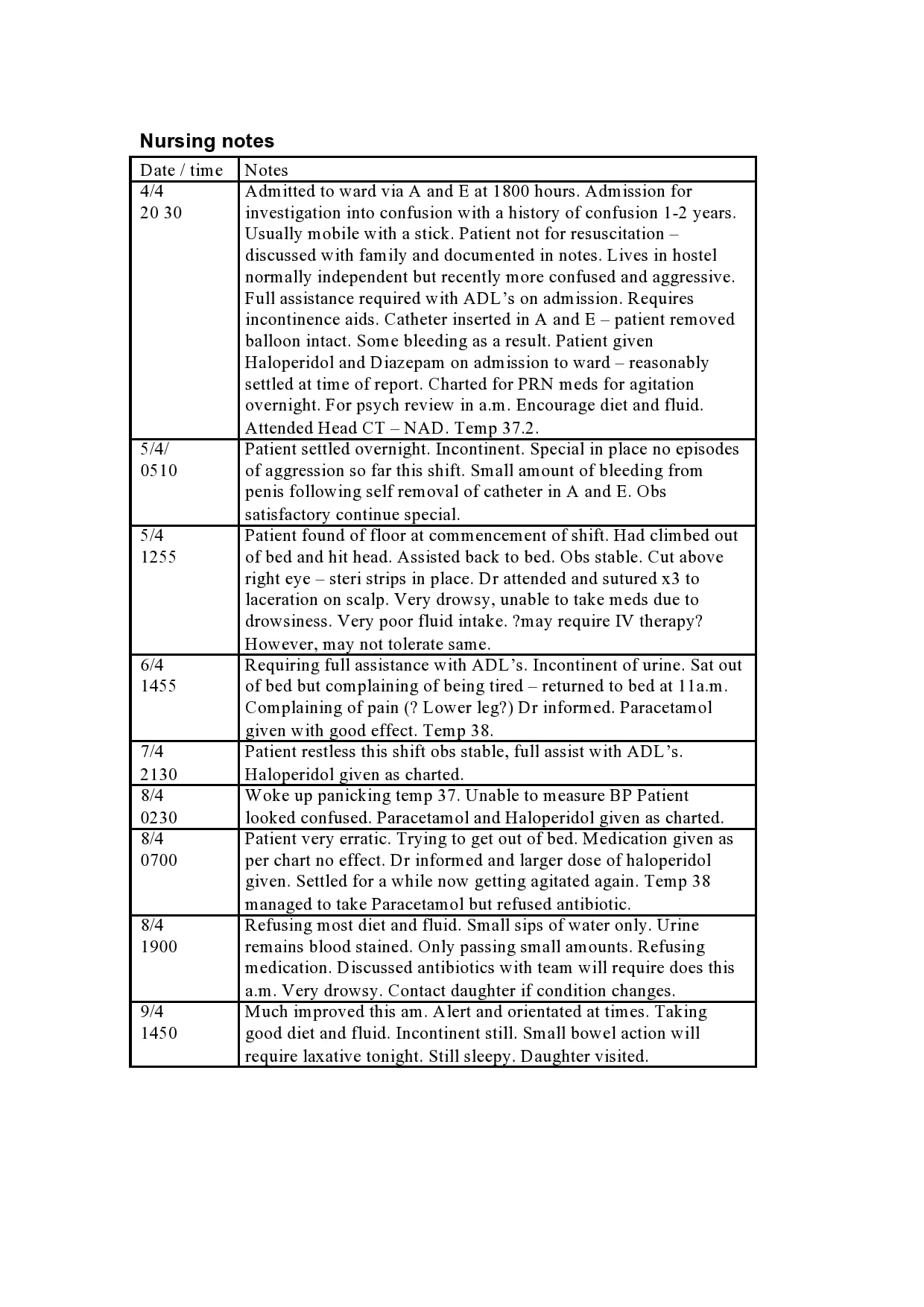
- Maintain consistency
The record starts with the ID information of the patient. Each entry should include the complete name of the patient, the time, and the date. - Write down timely information
You should write down your notes within 24 hours of supervising your patient. This means that you should have already accomplished the notes for the next nurse who will work the next shift. - Use legible handwriting
It is important that the notes should be both neatly and clearly written. Take your time when writing down your notes. - Opt for simplicity
Only write relevant information about the patient. These notes are supposedly designed for quick reading so avoid writing down lengthy details. - Document all of your communications
Remember to note down everything significant concerning the health of the patient. Every conversation you have with the doctors, family members, and any other medical professional you come in contact with. - Avoid using abbreviations
Write down everything in full. Abbreviations might mean different things to different people and this might lead to miscommunications. - Write as you go
As a nurse, it is your responsibility to complete all of your notes as soon as possible. This means that you shouldn’t leave your notes until the end of your shift.

")
