
As a health care provider, the records you take decide the level of care that your patients experience. Health professionals must provide notes that are detailed, succinct, thorough, and simple for other practitioners to use. In your patient records, using a pre-determined structure will help you improve the accuracy of your records. SOAP notes template is a form of measure of progression. Four components that fit each character in the acronym are included in the SOAP format: subjective, objective, assessment, and plan.
Contents
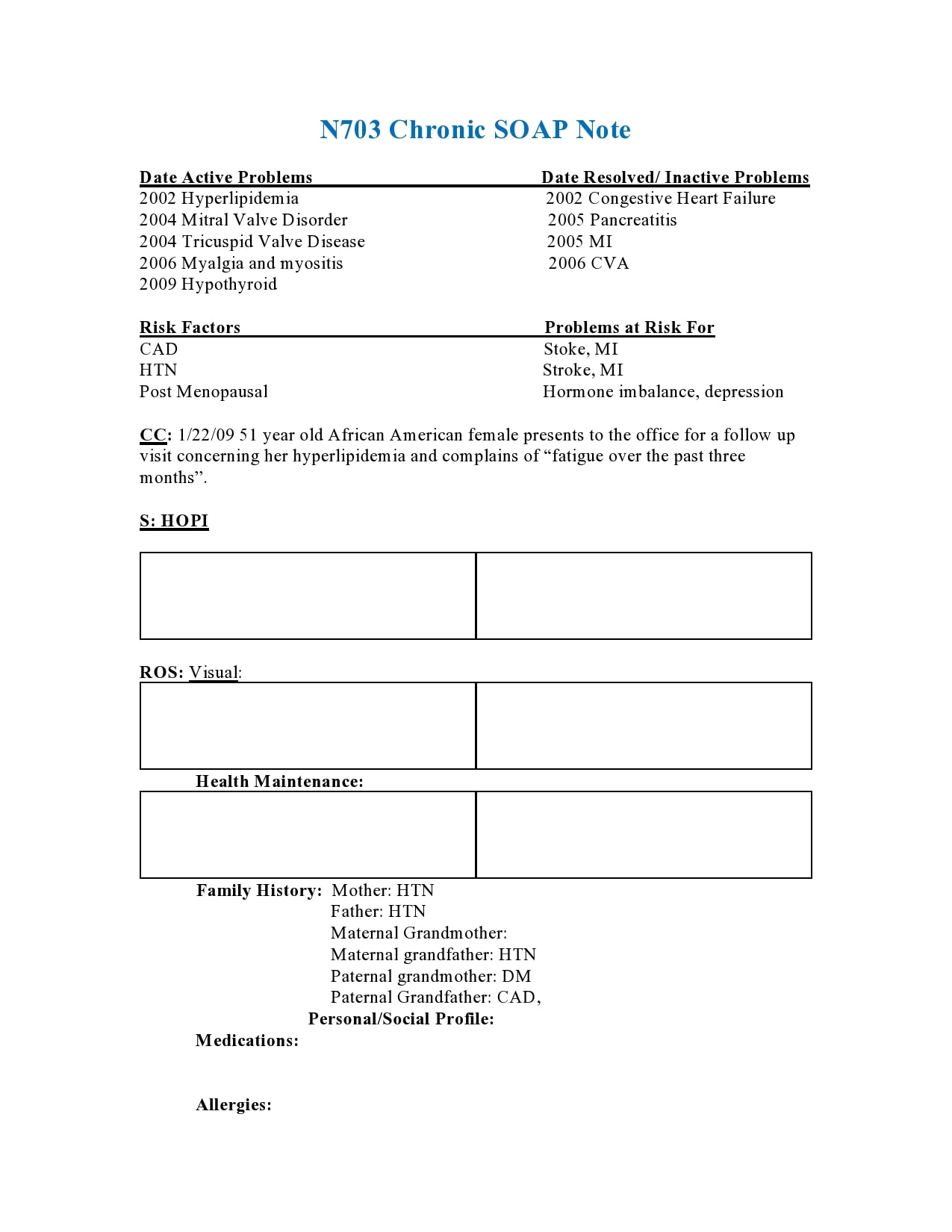
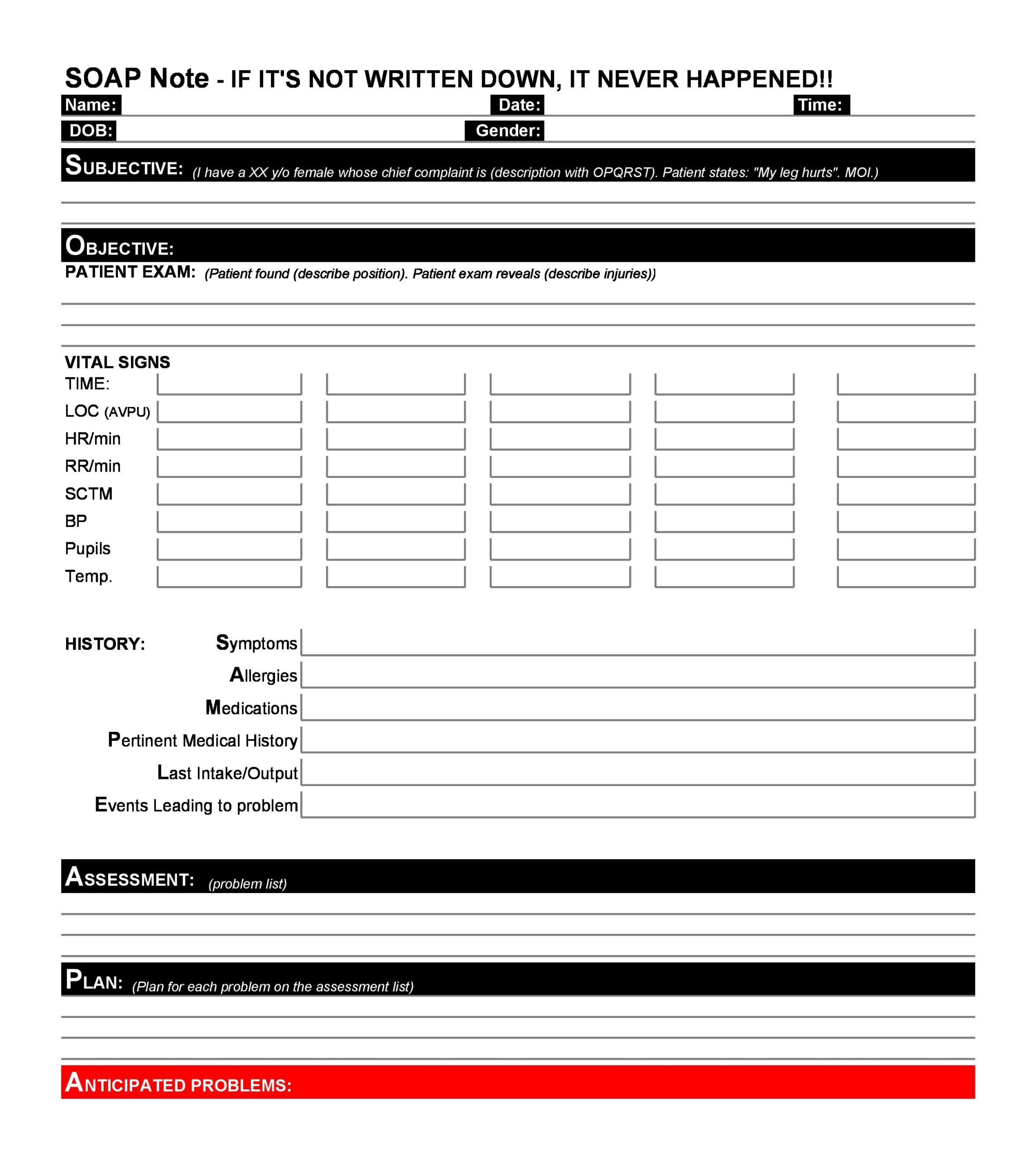
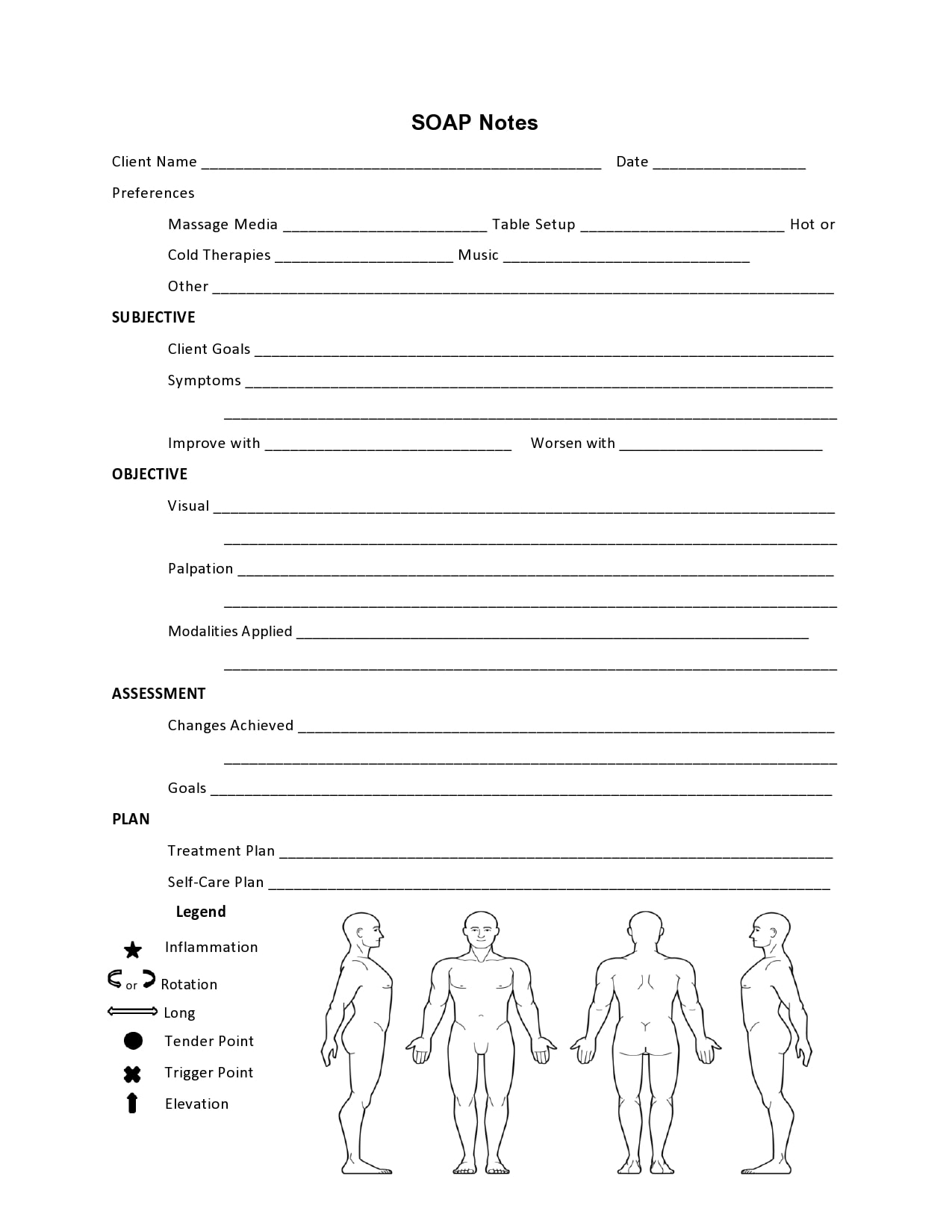
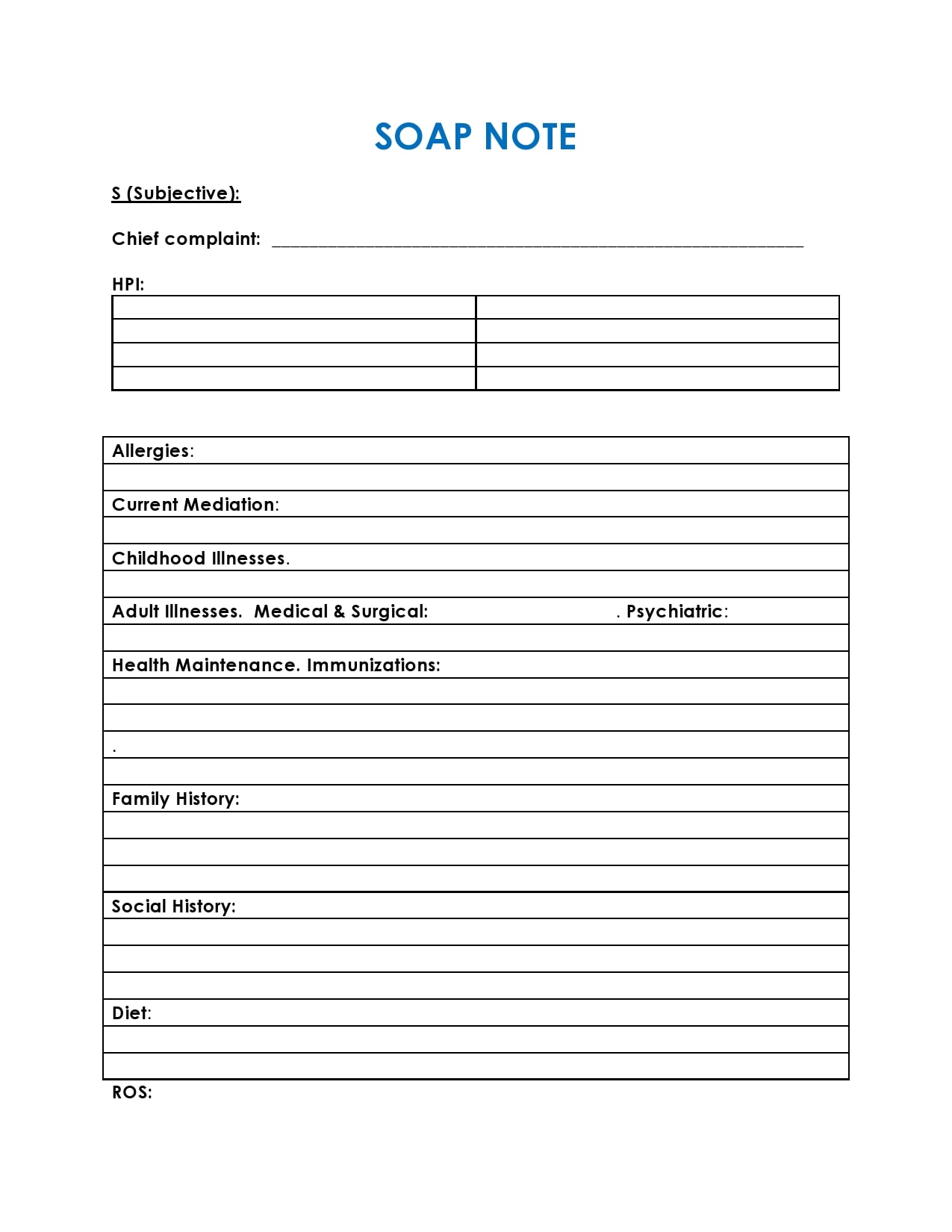
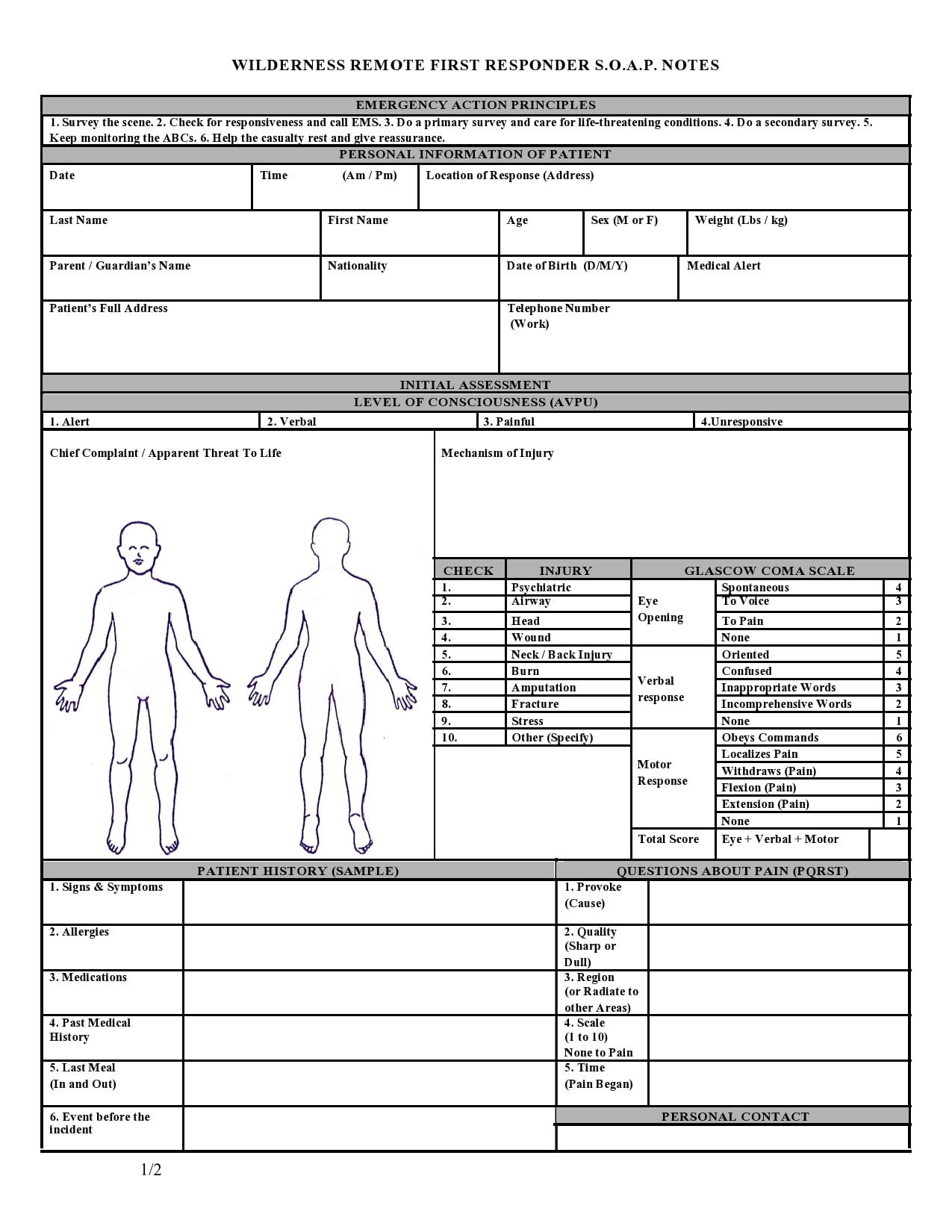
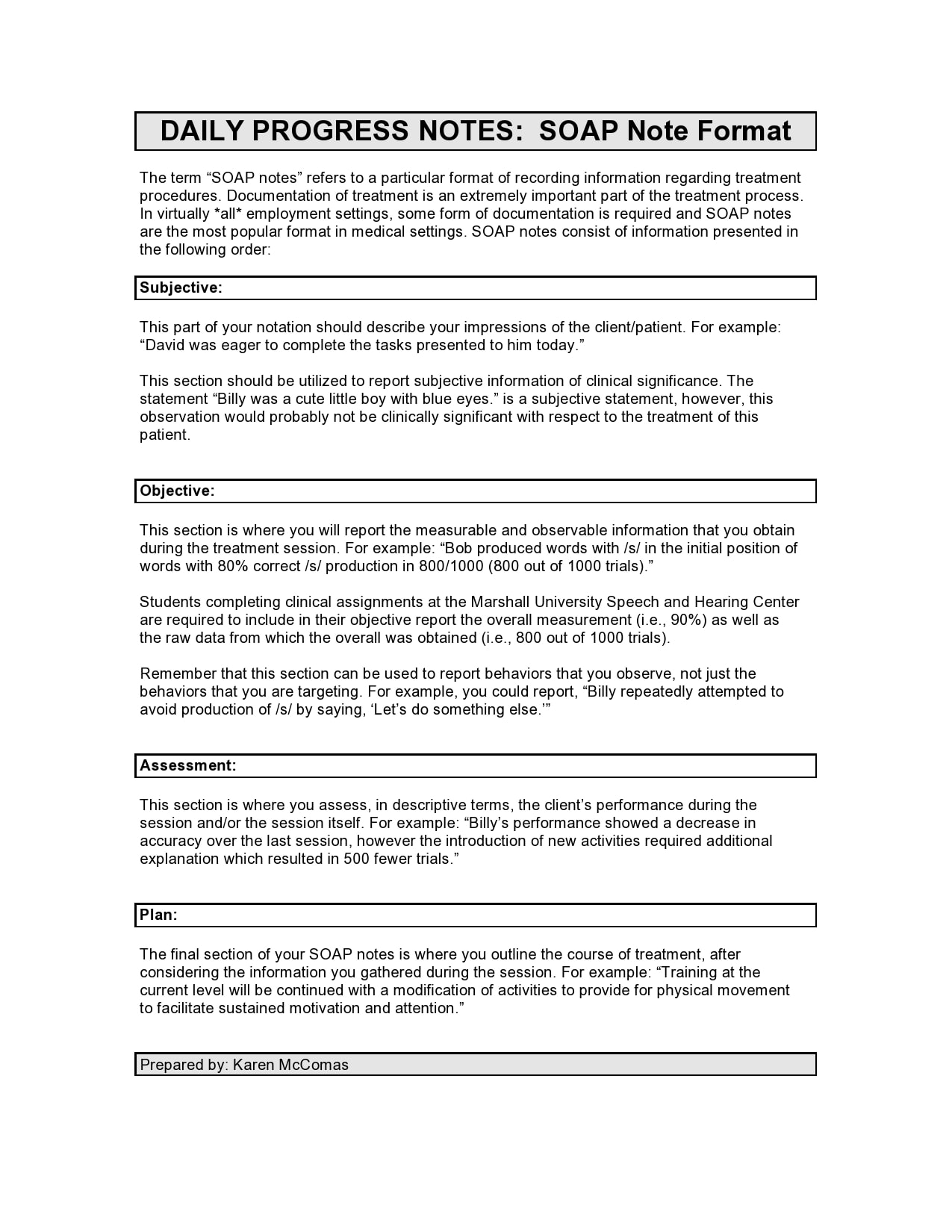
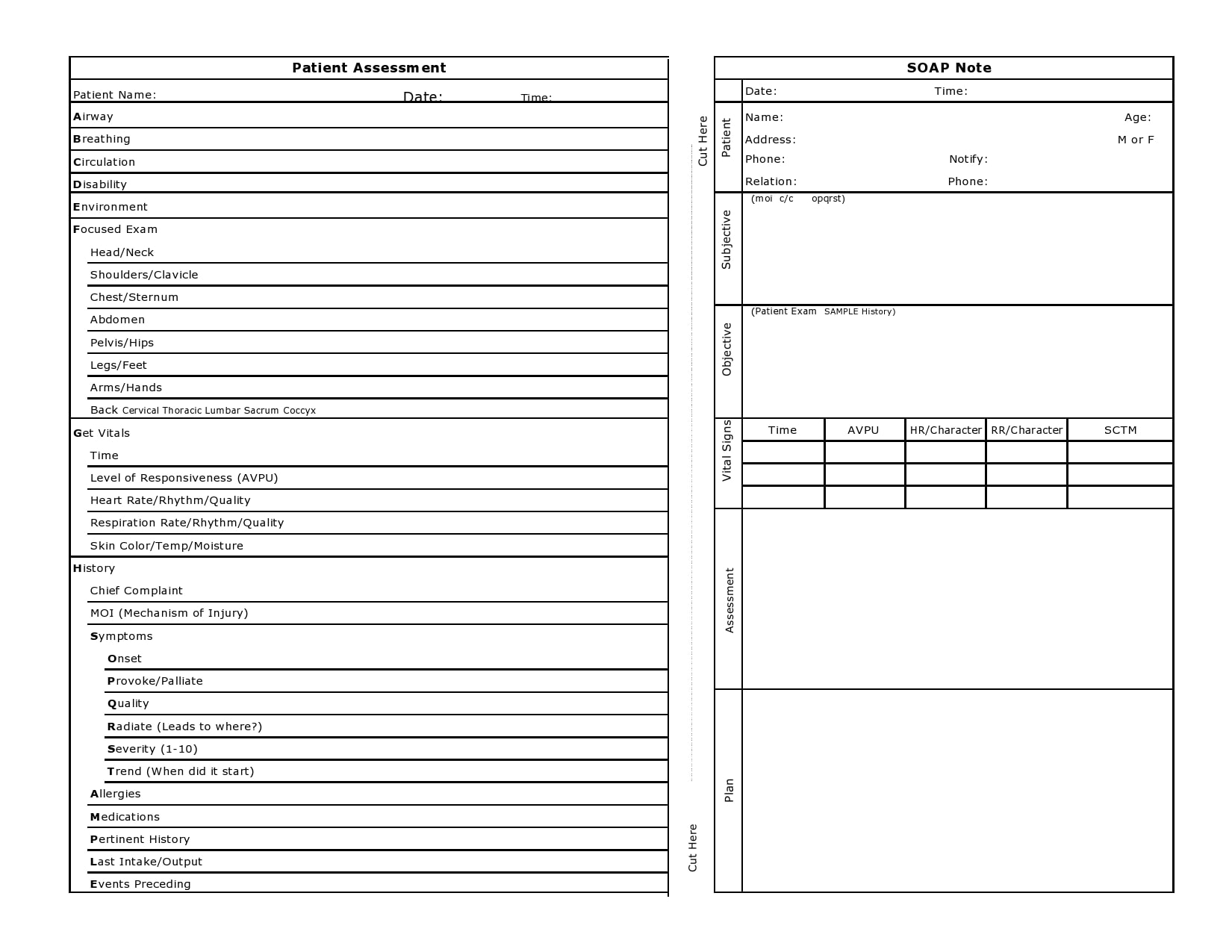
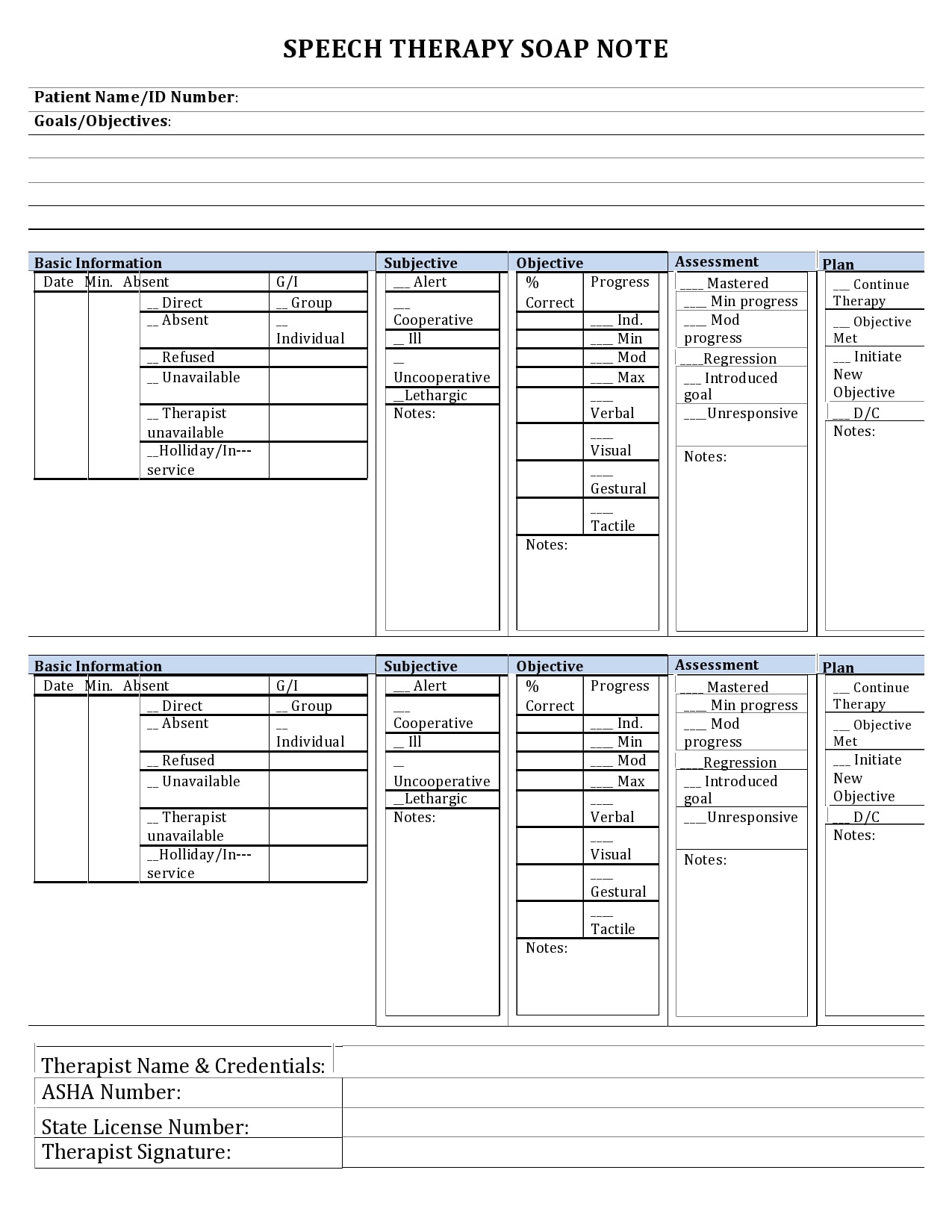
SOAP Note Templates

What do you write in a soap note?
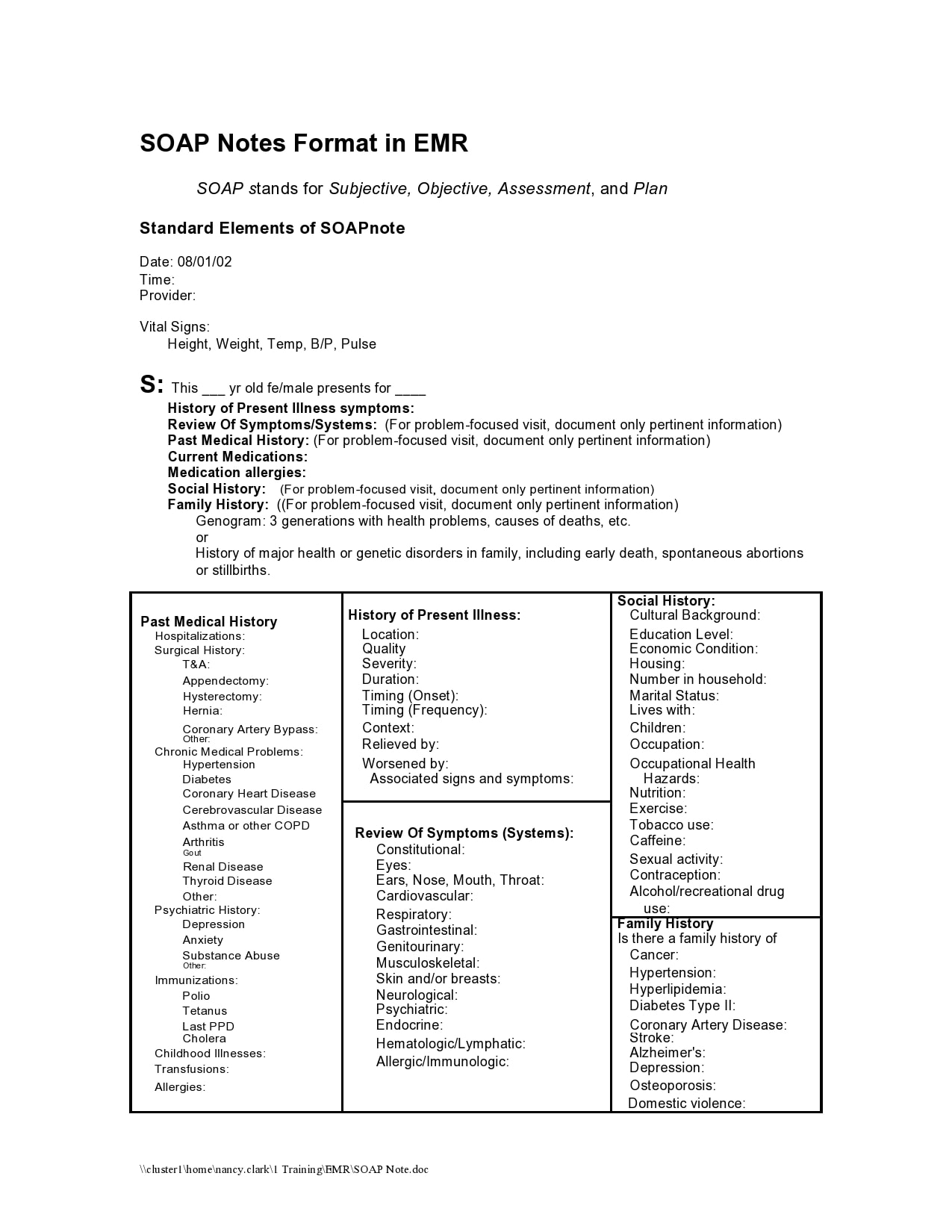
The SOAP note format helps medical professionals to record patient data easily through a highly structured style. This highly structured style often enables workers to easily find patient records and, when needed, retrieve key information
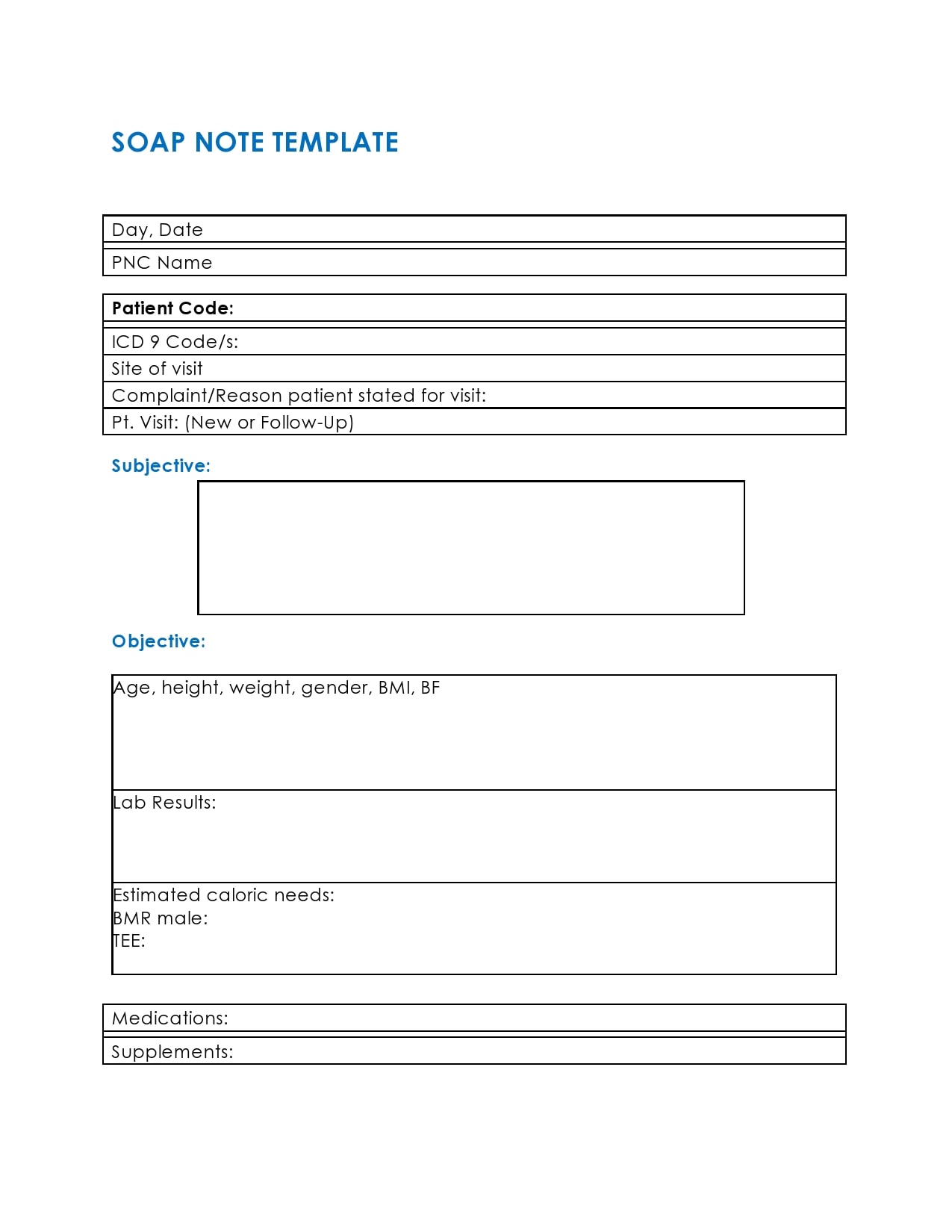
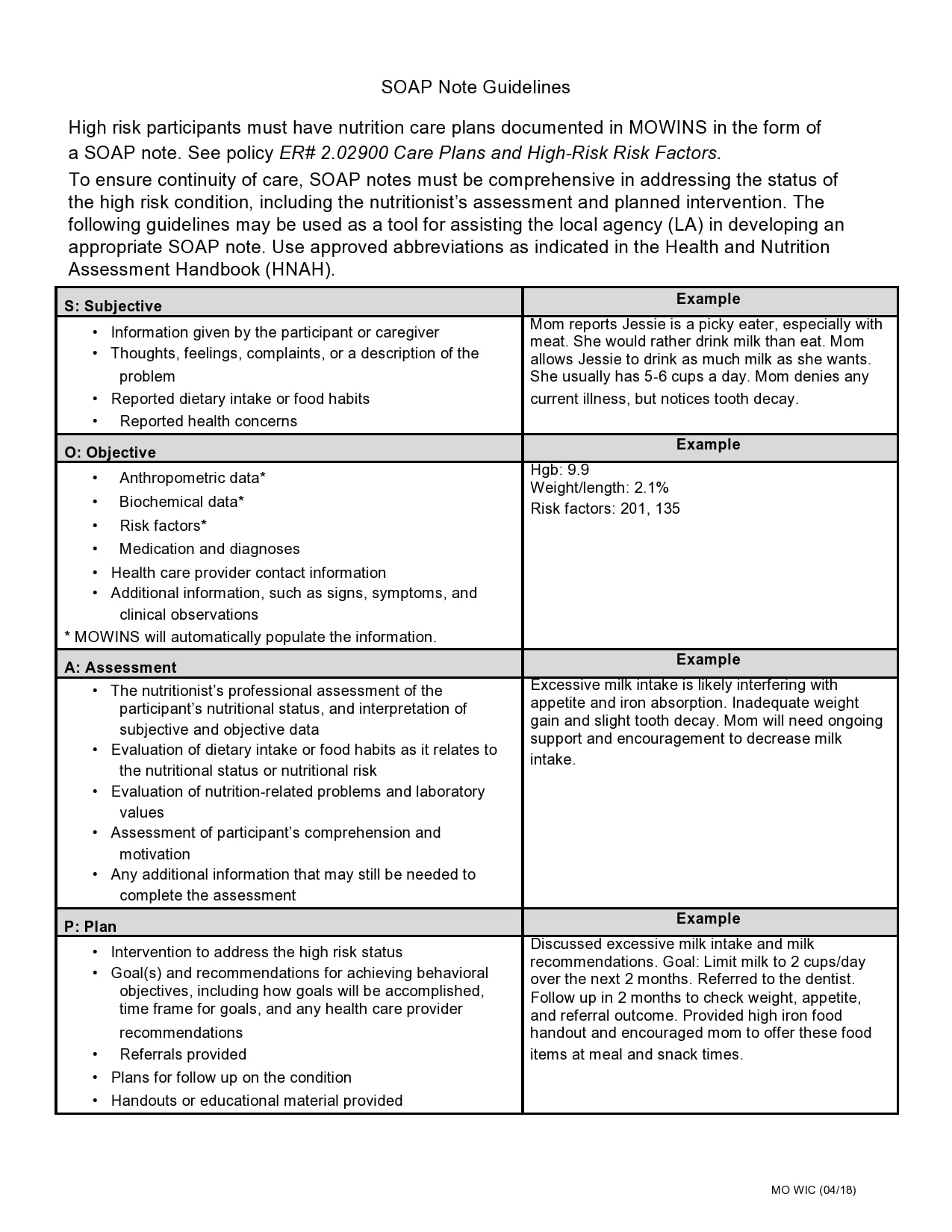
The medical professional must be guided by the four aspects of the acronym when inputting data. These four parts remind medical professionals of the data they need to obtain when appropriate care is needed. When writing in a soap note format, the four letters act as a guide to the medical professional.
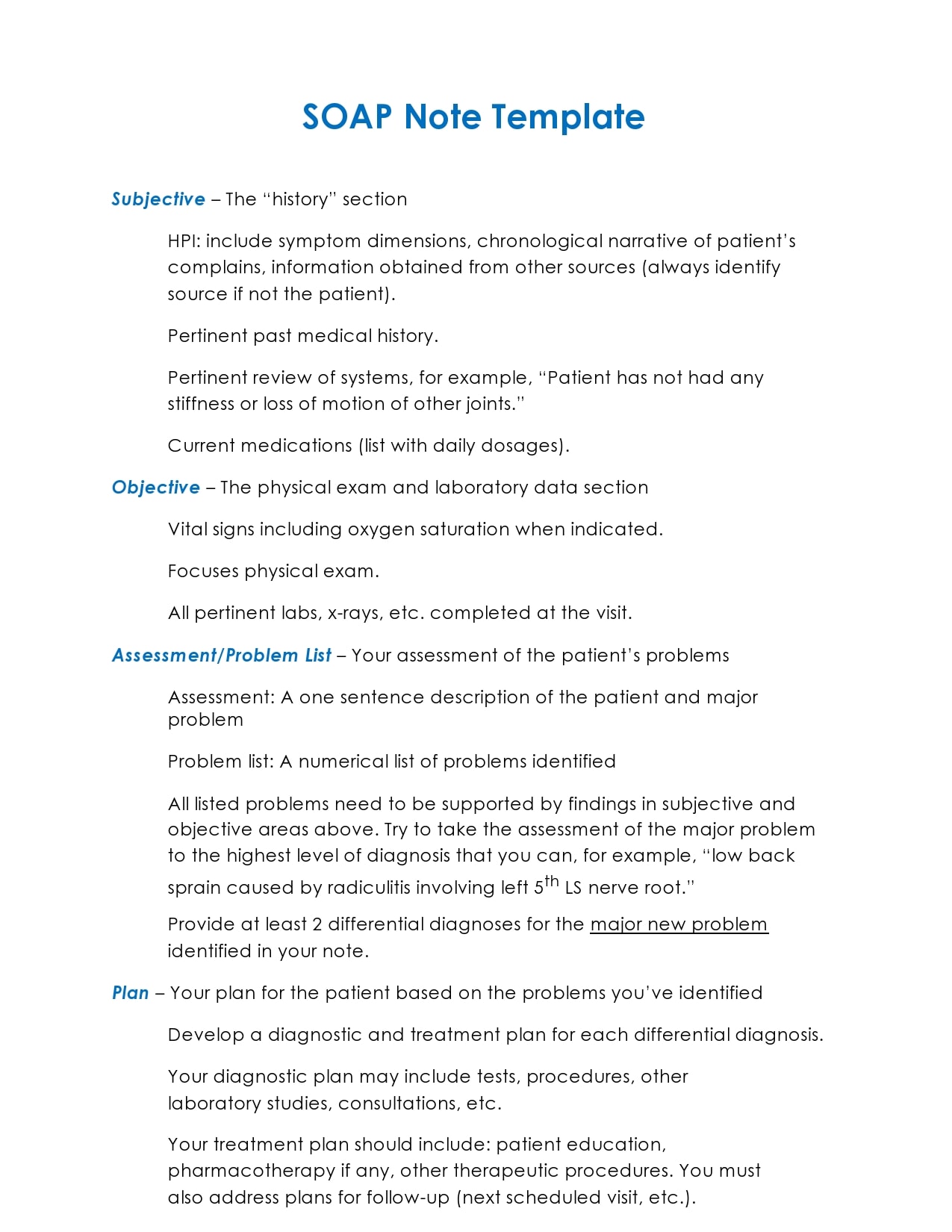
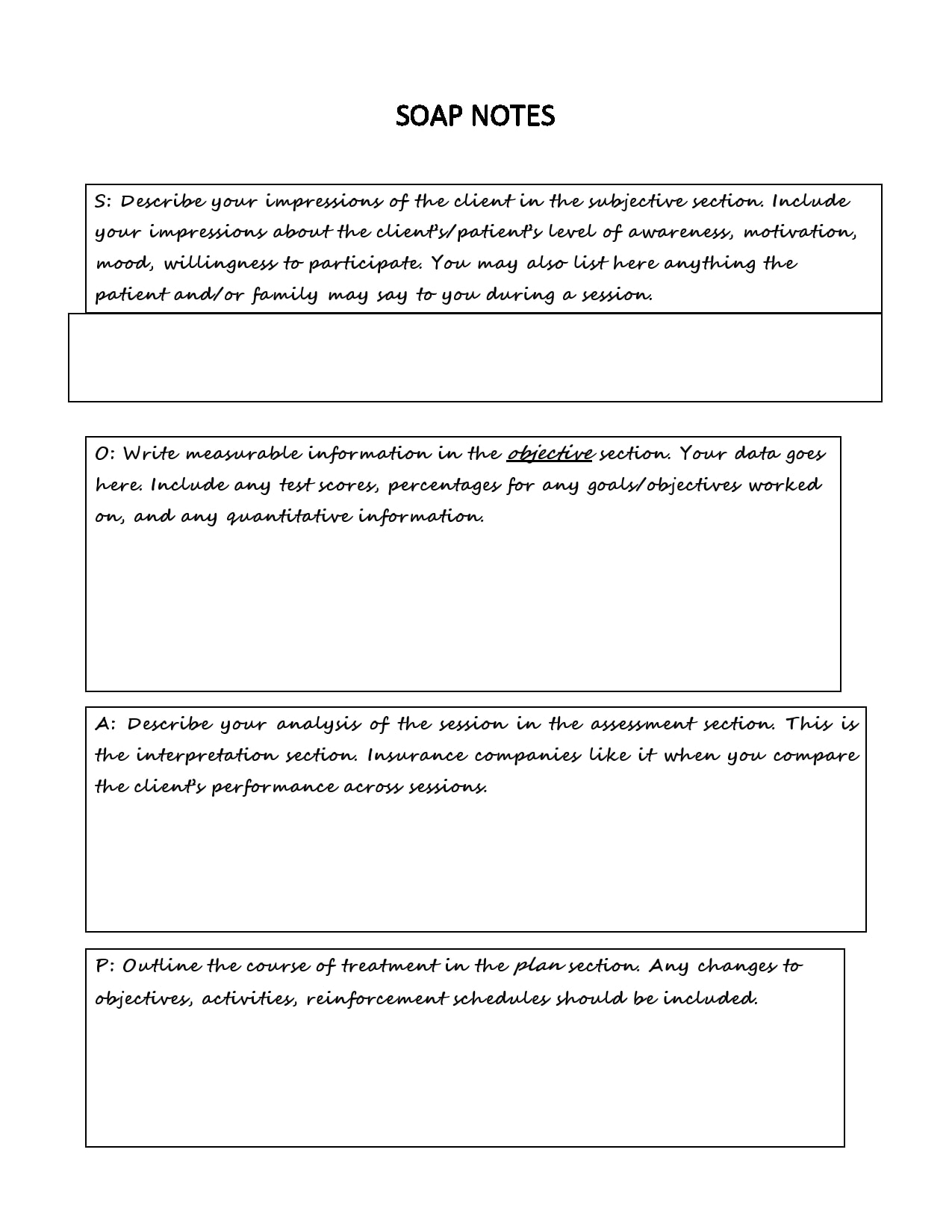
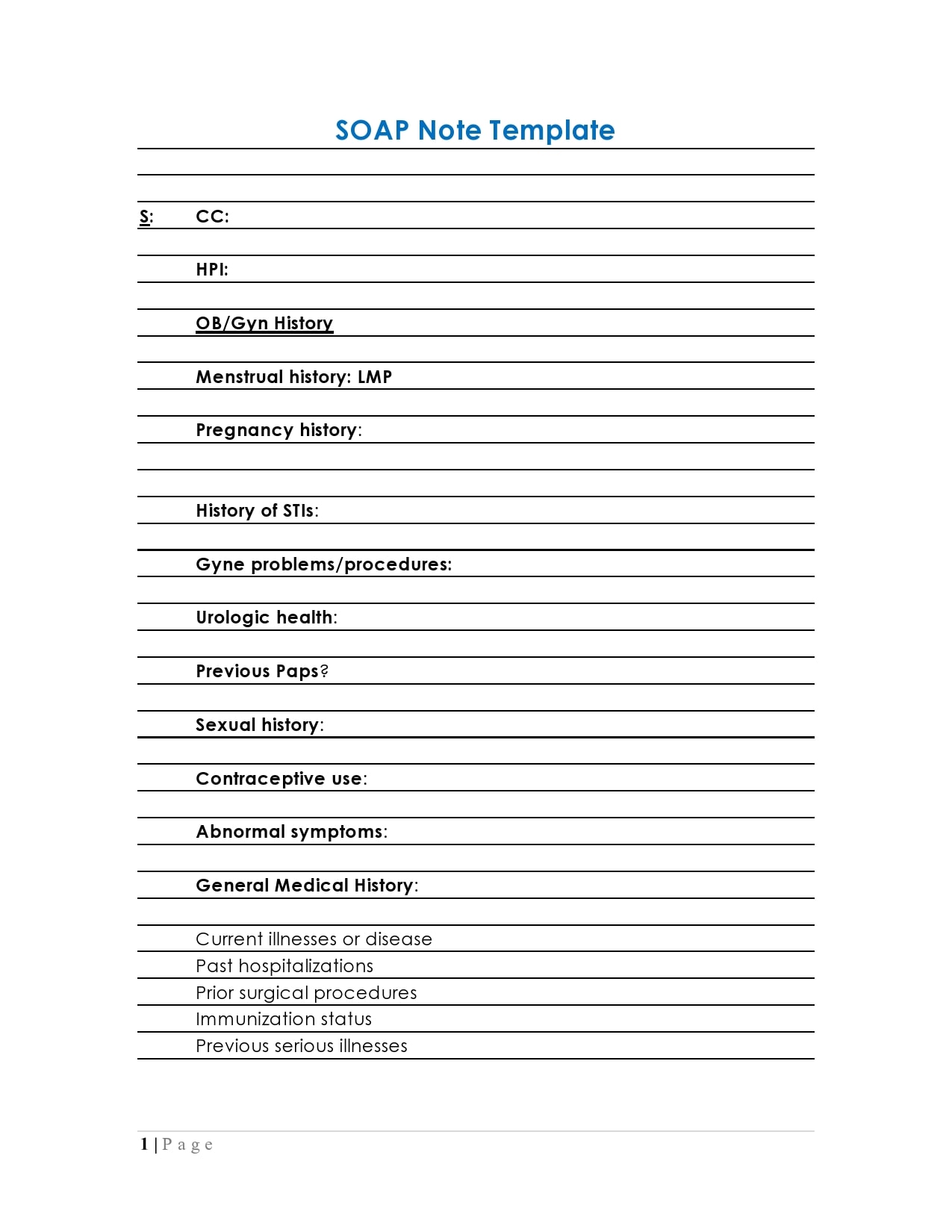
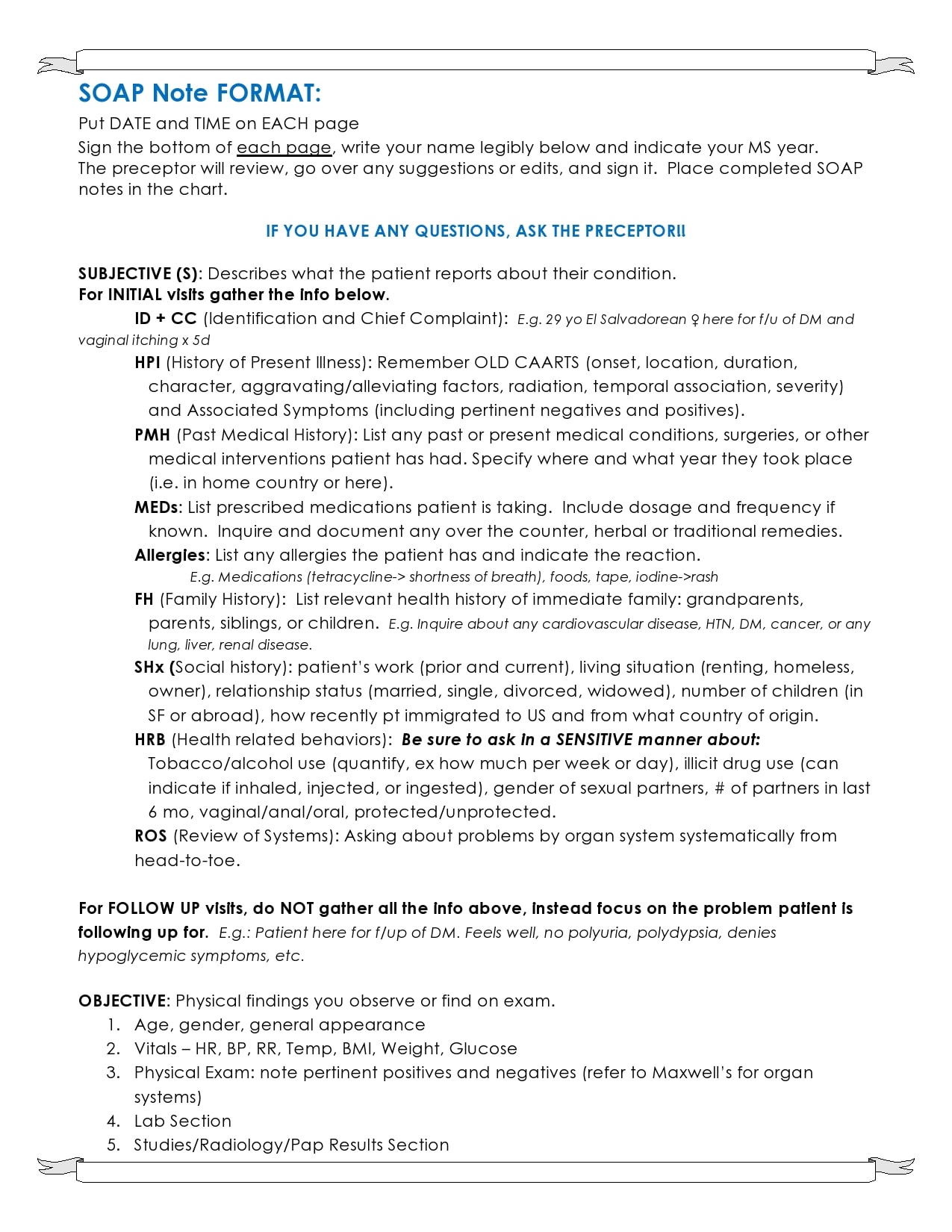
- Subjective
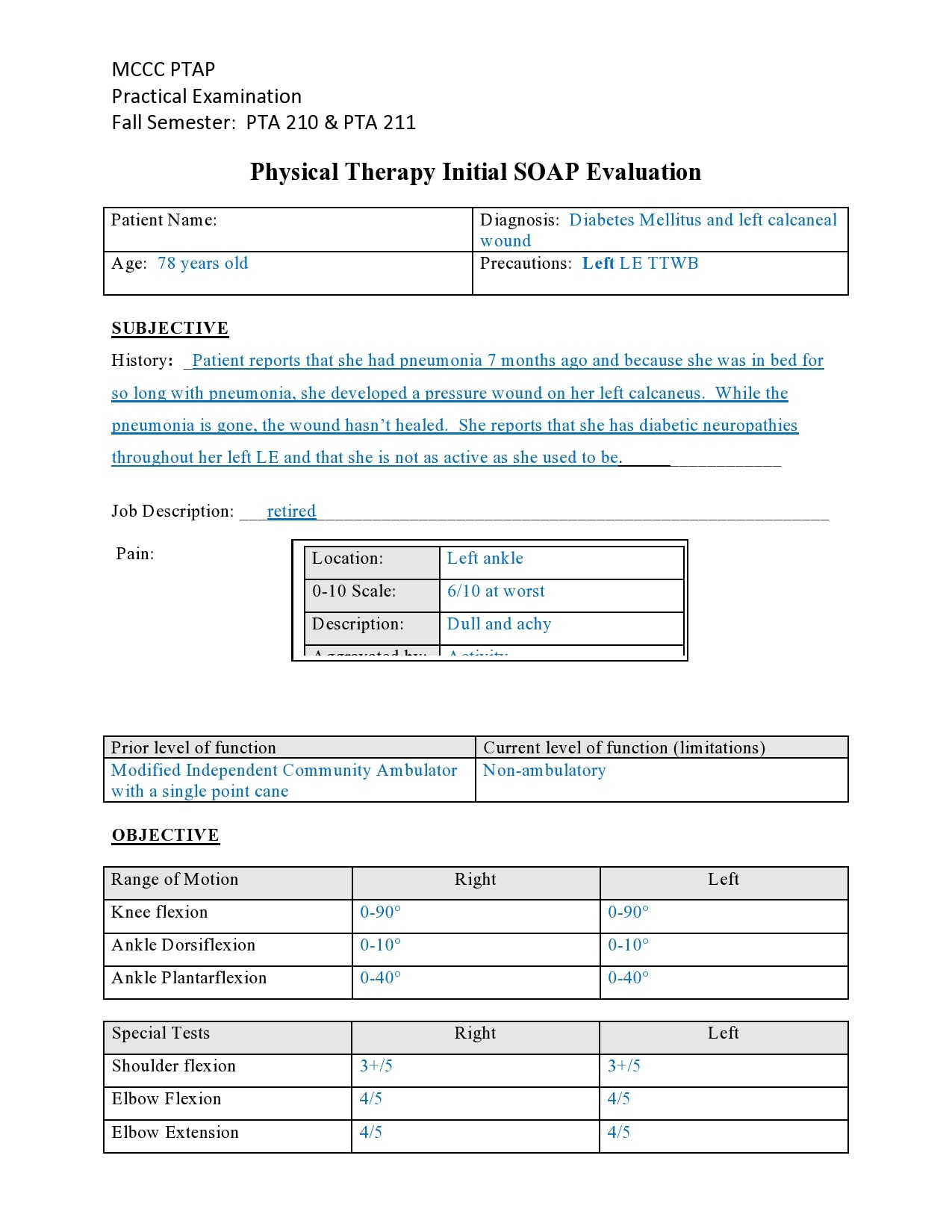
The first step is collecting all the details concerning the symptoms that the patient has to disclose. The client will inform you regarding their history with the symptoms associated, and also what their care expectations and priorities are considered to be.
The Selective Description must include specific patient references. A patient, for instance, could say, “I would like to speak concerning my frustration with my son.” This word by word quotation will be added by the therapist. Instead of rephrasing words, it is essential to document the words of the client, so you create the clearest insight about their situation.
The suitable position for listing any sentiments expressed by the patient, any relatives, or their caregivers is also the Subjective segment. This classification is the framework for the remainder of your notes as well as your treatment plan, so it is important to obtain the best quality data possible. The sample SOAP note acronym offers a clever way to thoroughly address the emerging situation of a patient.
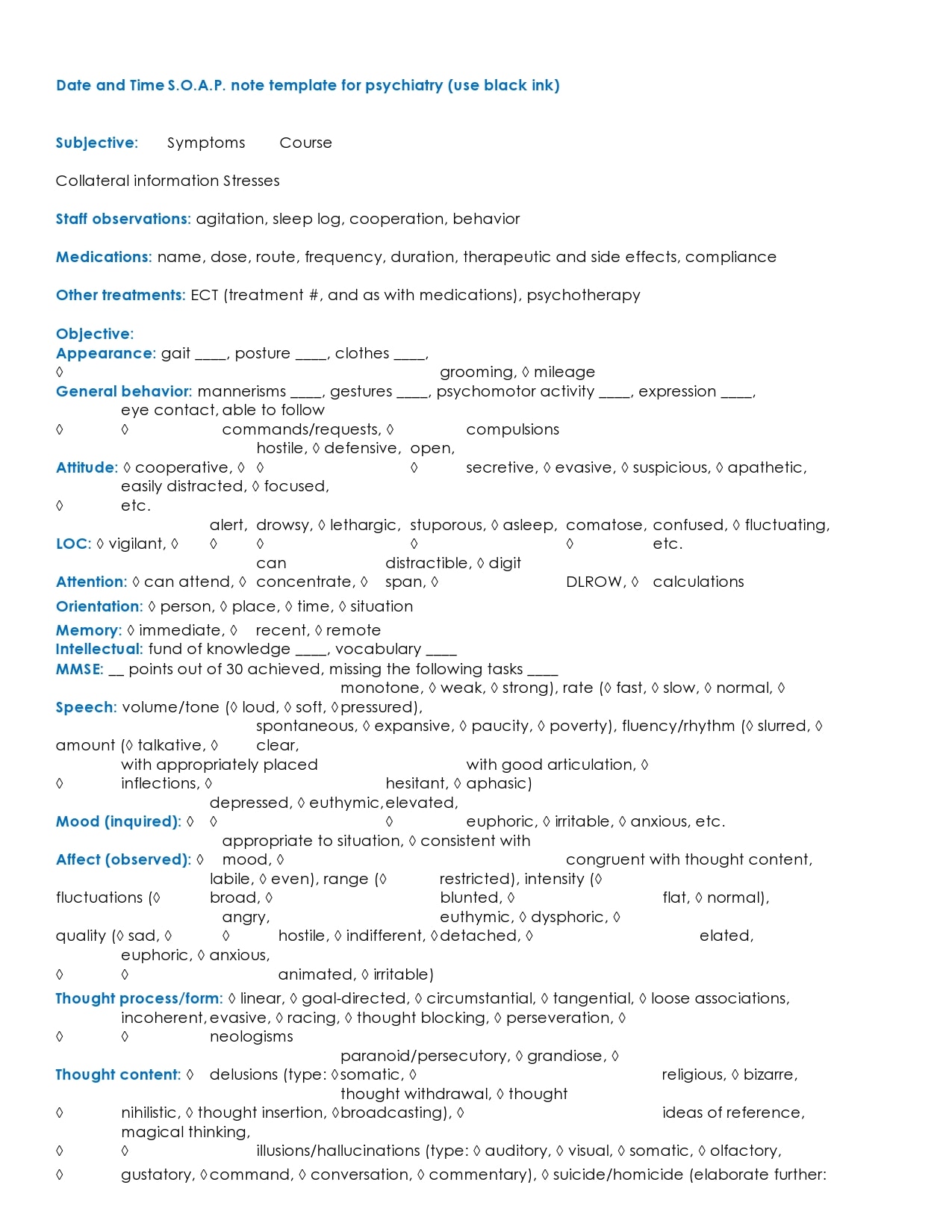
While physical information does not always require to be provided in the SOAP note format for mental treatment, the SOAP note template can be useful to therapists if they coordinate treatment with another health professional’s client.
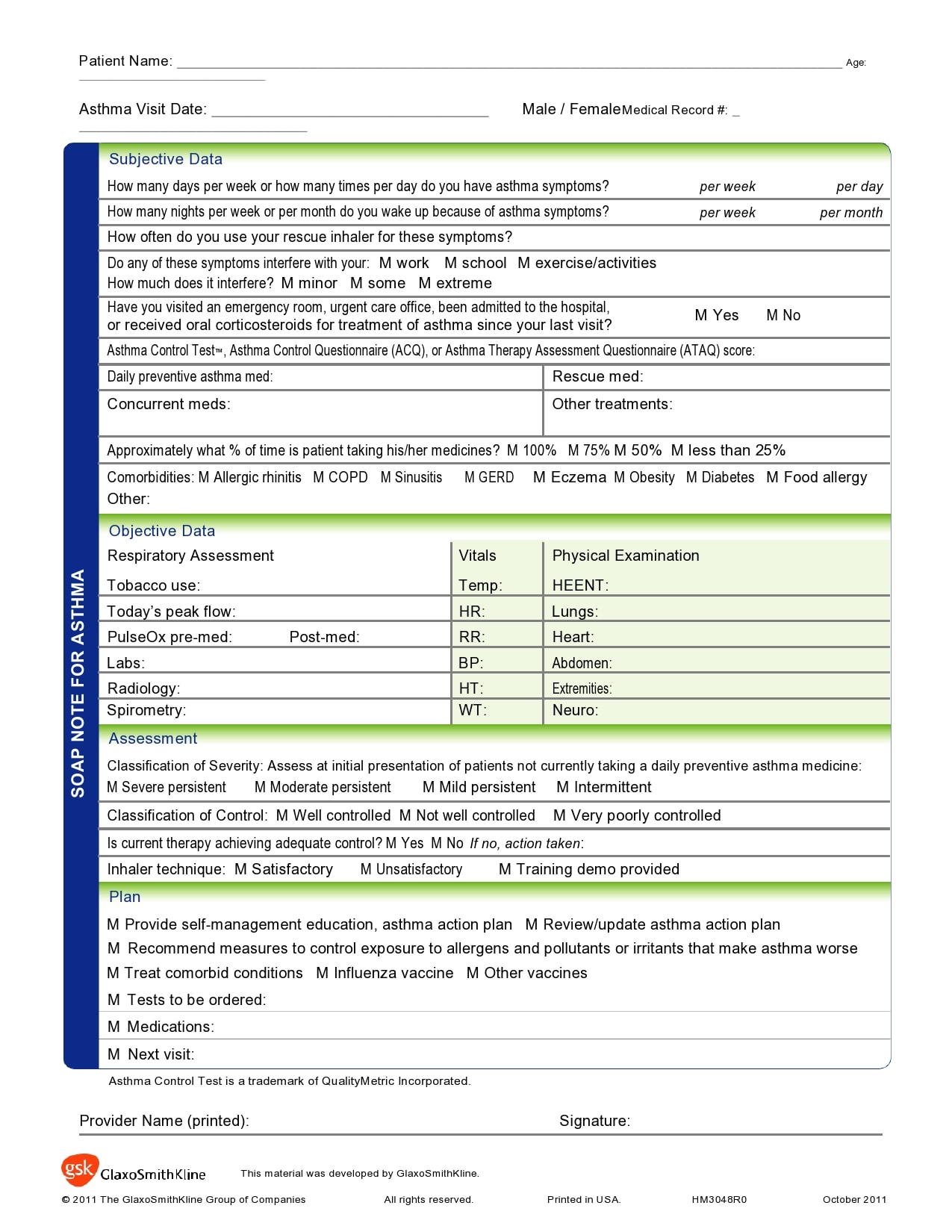
Psychological wellness and general wellness are interconnected, and one affects the other very frequently. For example, up to 34 percent of heart failure patients experience depression, as per the American Heart Association. Consequently, the subjective component may also be used by mental health providers to identify any physical symptoms that a patient may show. - Objective
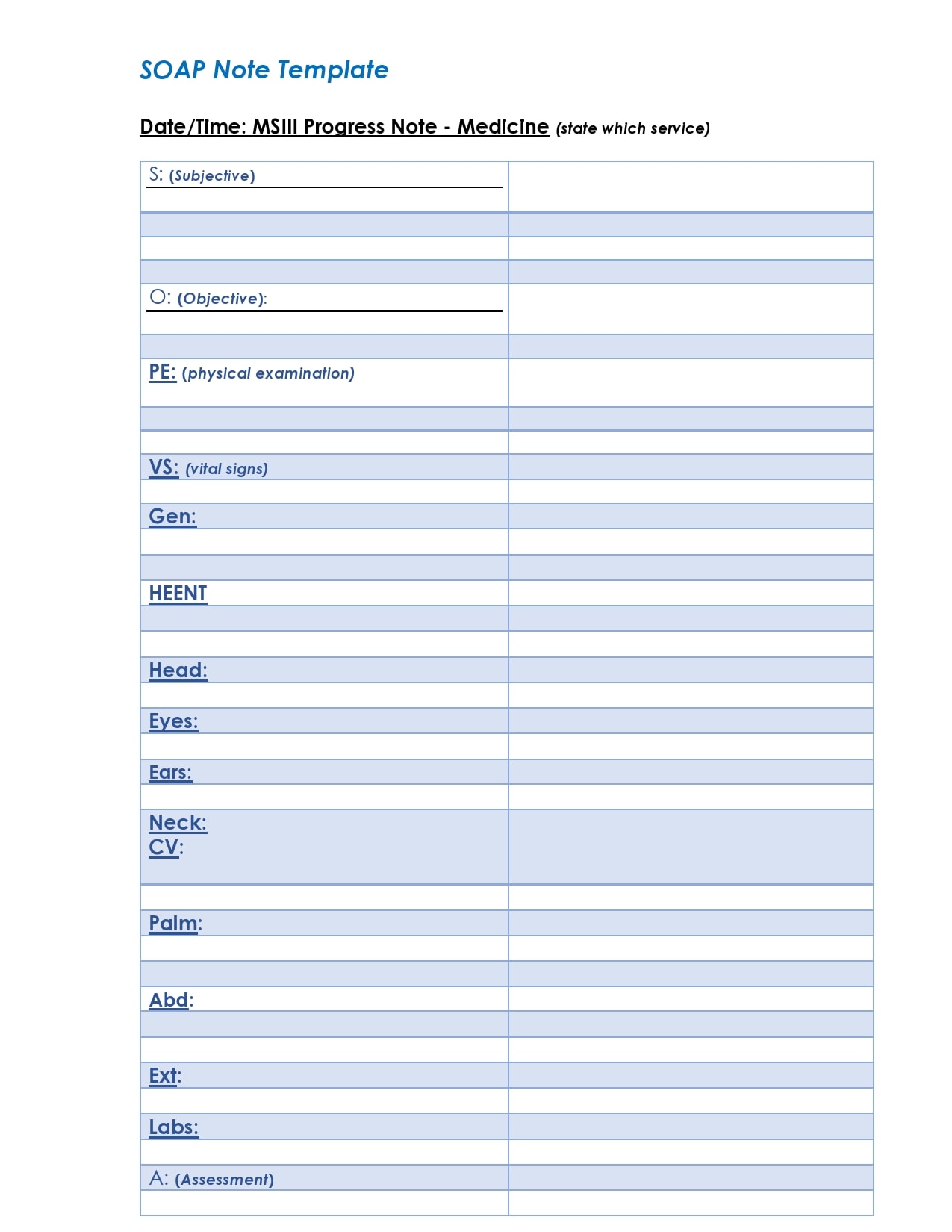
A SOAP note’s objective section contains realistic facts. Detailed findings concerning the look, actions, physical expressions, and emotions of the patient could be included. You could report, for instance, that the patient came to the therapy 20 minutes late and slumped on the bench.
Note down the specifics as cleanly as possible. The objective stage is just about unprocessed data, on your part, and not assumptions or evaluations.
Record any observable results, along with appropriate examination reports, during the patient consultation.
The problem of distinguishing symptoms from signs is solved by recording the Objective notes. Symptoms are the perception of their illness by the patient, whilst signs are concrete diagnosis findings.
If a patient claims feelings of depression, like anxiety disorder, signs of nervousness may include noticeable muscle tension or twitching, as well as physical test-determined high blood pressure. You have a short review window, so it is necessary to deliberately search for any indicators that support or refute the details outlined in the sample soap notes’ subjective portion. - Assessment
In the evaluation process, both the subjective and objective aspects reported earlier come into play. Based on the information you’ve obtained, you can record your observations and make conclusions.
For first visits, an assessment centered on the nature and magnitude of symptoms identified and signs witnessed could or could not be included in the evaluation section of your soap note format.
The examination is fairly simple for general disorders such as depression and will often result in a diagnosis within the initial or two visits. Before resulting in diagnosis, you might require extra space to gather data on the subjective and objective levels for rarer and very complicated disorders or the others which appear co-morbidly.
The Analysis section of SOAP format notes contains an assessment as to how the patient is doing towards defined recovery objectives for follow-up appointments. Based on how the patient is reacting to therapy as intended, the evaluation will advise the ongoing therapy path as well as plans for the future.
It is necessary to focus on if your patient is exhibiting progress, sustaining progress already achieved, deteriorating, or showing regression trends.
Your evaluation can only include as much detail as is required, like the other parts of SOAP notes. Based on the severity of the patient’s situation, some tests can take considerably longer than others. Often just a few bits of details would be included in this part of your notes, such as, “Patient sleeps better, no improvement in the frequency of anxiety disorder.” - Plan
The plan section is the stage from which all the three preceding parts arrive together to assist you in determining the path of subsequent therapies. Details on the plan segment of your SOAP notes typically includes information on:
At the session, the prescription was provided and your reason for prescribing rationale.
The initial reaction by the patient to the medication
What’s the next appointment for the patient is
Any guidance you offered to the patient, especially homework tasks
Objectives and result indicators for re-assessing new challenges or problems
With each diagnosis, the SOAP plan format should include measurable objects. If your patient experiences several symptoms in tandem with a drug use disorder, such as post-traumatic stress disorder, your findings must contain distinct measures for each diagnosis.
The purpose of this segment is to resolve all the particular drawbacks mentioned in the report. If performed successfully, the sample SOAP note creates a clear path for the continued care of the patient and allows all physicians to draw perspectives to extend the treatment if necessary. With each successive visit, review the plan and change it periodically in the light of the recommendations in the evaluation section.
SOAP Note Examples


How is the SOAP note used?
- During rounds
You may not hope to recall specific details about every patient admitted to the health care center like laboratory tests, and important signs. It will be appropriate if you refer to your SOAP note example.
Organize your ideas before you compose your notes. You may not need to write everything, for instance, in a similar order as the patient stated it. Allow a couple of moments to reflect on what and in which manner you would like to document what you need to include.
Disregard Contributive Data. You already have sufficient facts to report, and it does not benefit to incorporate details that are not important to the circumstance. For instance, if you state that patients have no discomfort, you don’t have to cite their exact comment. - Follow-ups visits
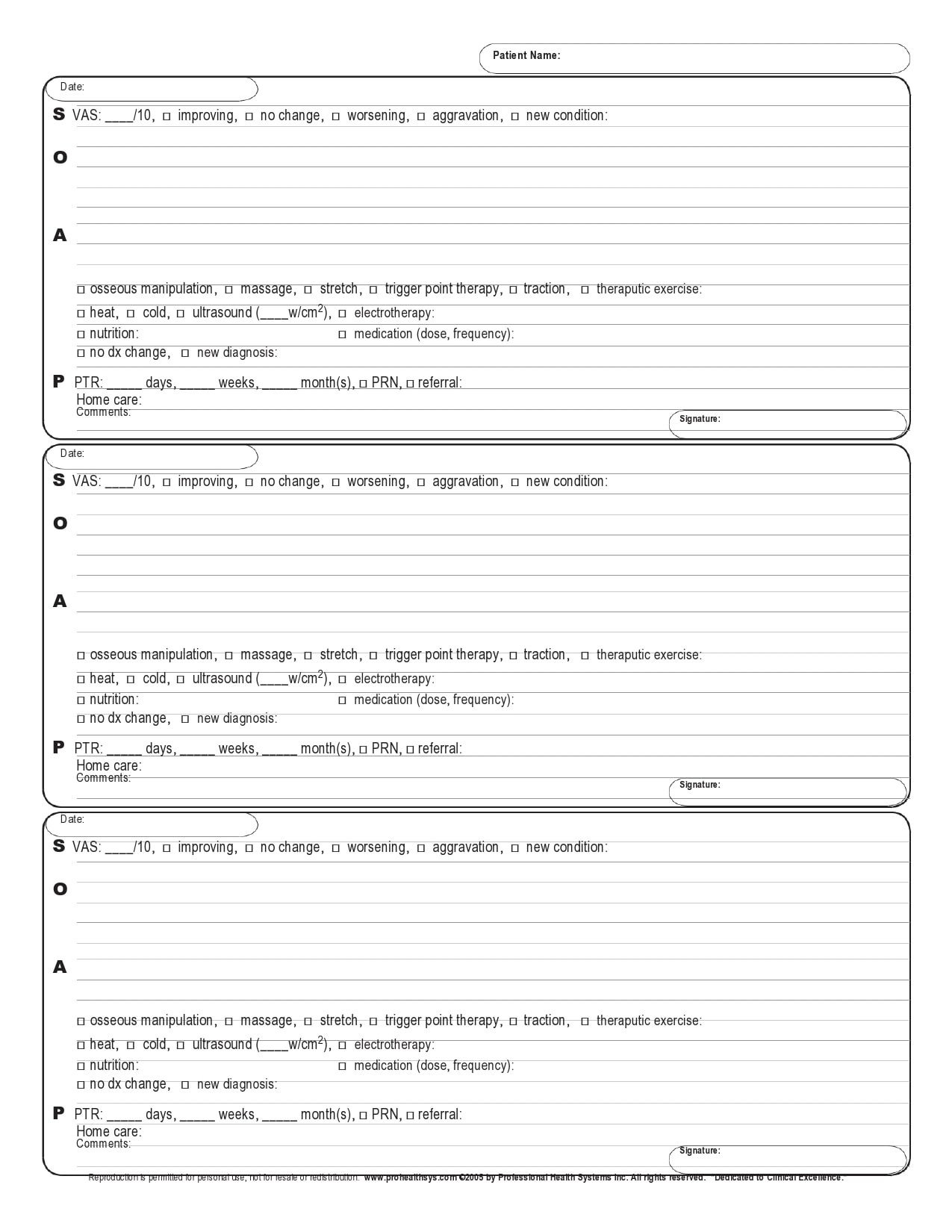
During follow-up visits, the physician keeps referring to the soap note to check the history of the patient. The physician examines the condition of the patient in comparison with the condition they were in the last visit.
Based on the available data, the physician can come up with a new set of questions to examine the response of the patient to recommendations and treatments. The physician will add the new information obtained from the patient in the SOAP note format. - Diagnosis
The physician can use the information contained in the SOAP note to set the steps for relevant diagnostic procedures for the patient. From the information in the SOAP note, they may recommend the patient to another specialist for further observations.
The physician may also recommend certain tests or exercises to the patient-guided by the information in the SOAP note. - Share information
The soap note sample can be used to share information between specialists. If a different specialist needs to check on the patient, the information contained in the SOAP note will be useful.
In the absence of the patient’s physician, the physician on duty can use the information in the SOAP note to refer to the history of the patient and be able to catch up without hindrances. - Treatment
The SOAP note example can be useful during the treatment of patients. When the data in the SOAP note format is combined with diagnosis results, the physician can prescribe an effective treatment for the patient.
In other words, the treatments and cures for patients shall be as accurate as possible when the correct information is recorded in the SOAP note. The result of accurate treatment and cure measures means the patient will respond positively and quickly to any drugs prescribed or to any other therapeutic recommendations the physician may prescribe.
Any subsequent treatment of the patient can be tied to the recommendations contained in the plan segment of the SOAP format note towards effective and quick recovery.
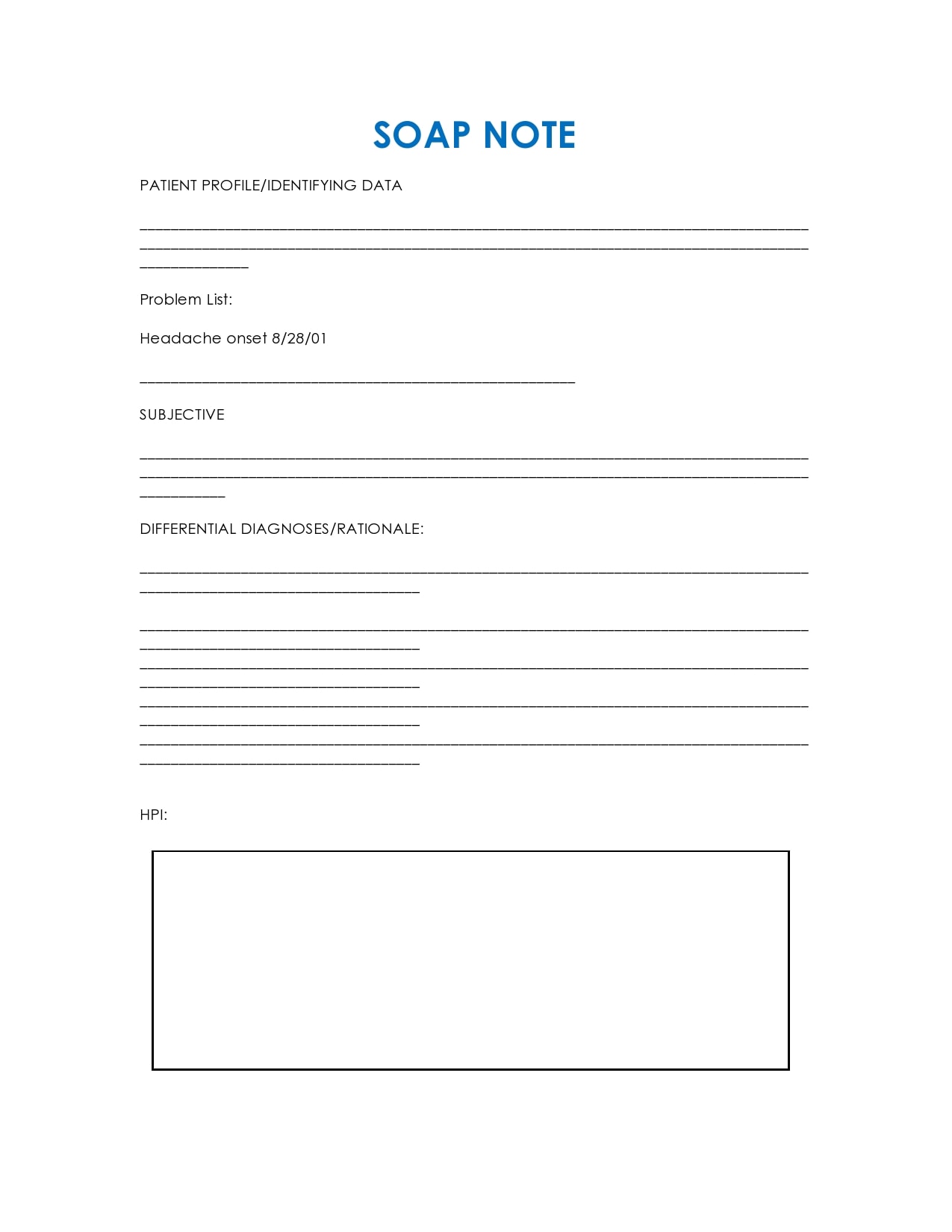
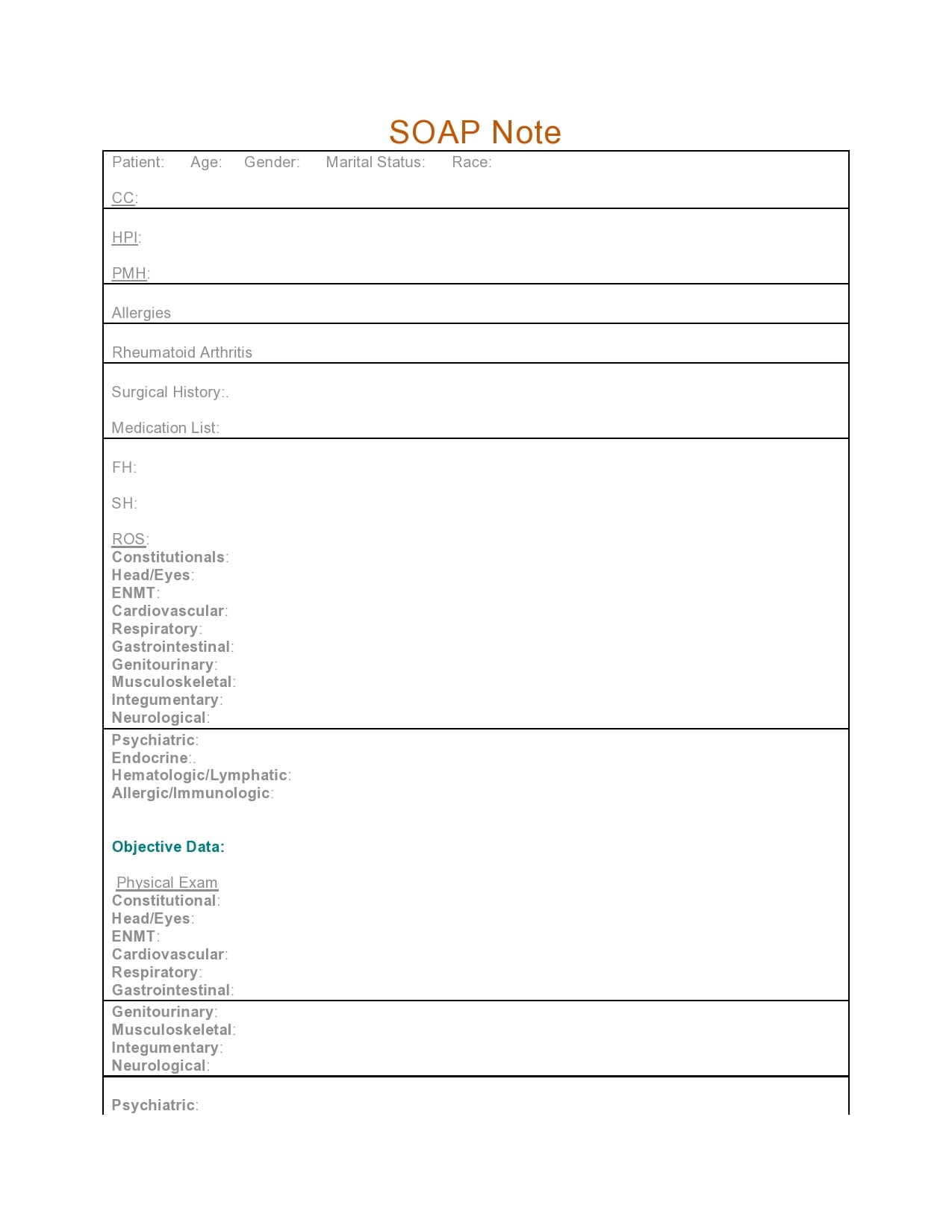
SOAP Note Format

")
